Bpc-157 Injection Method Subcutaneous bpc-157 injection method subcutaneous or intramuscular How Do You Take BPC-157? Injection, Oral & Dosing Guide
If you’re trying to figure out a bpc 157 injection method subcutaneous vs. intramuscular approach, you’re probably running into the same problem I did the first time: conflicting dosing instructions, unclear injection technique, and a real fear of getting it wrong. This guide is written from a practical, hands-on perspective to help you understand the injection choices (subcutaneous and intramuscular), what those routes tend to mean for absorption, and what a safer decision process looks like before you ever draw a syringe.
Important: BPC-157 is not an approved medication for general human use in many places, and dosing/injection guidance online is inconsistent. I’ll cover what to consider (and what to avoid), but you should use this information only to talk through options with a licensed clinician who can assess your health, risks, and the specific product you have.
What “bpc 157 injection method subcutaneous” really means
When people ask about the bpc 157 injection method subcutaneous, they’re asking about the route of administration—where the injection is placed in tissue. Two common routes discussed online are:
- Subcutaneous (SC): into the layer of fat just under the skin.
- Intramuscular (IM): into muscle tissue.
In my experience (including managing injection routines for myself and supporting teammates who were training protocols), the route matters because it changes:
- Tissue absorption dynamics: SC often spreads through fat planes; IM is deeper and typically has different blood flow patterns.
- Local tolerability: some people report different levels of soreness, swelling, or bruising.
- Injection technique complexity: IM usually requires more precision regarding depth, angle, and avoiding nerves/vessels.
Subcutaneous vs intramuscular: choosing a route responsibly
Both routes are described online for BPC-157, but the decision should be clinical and individualized. Here’s how I’d compare SC and IM at a practical level—focused on technique, risk, and “what changes when you move the injection deeper.”
Subcutaneous (SC) injection: what it’s like in practice
In SC dosing, the needle enters the sub-dermal fat layer. The technique is often taught as a pinch-and-insert approach on certain body areas. In my hands-on work with routine self-injection education, SC injections generally feel more controllable for many people because the tissue plane is more forgiving—though the downside is that some people still get localized irritation.
Typical practical considerations:
- Needle length and angle: should match body habitus and product formulation—using an inappropriate needle length can increase discomfort or risk.
- Site rotation: rotating SC sites reduces repeated trauma in one spot, which can minimize lumps and bruising.
- Reaction monitoring: SC can cause redness or a palpable bump; that’s a reason to be deliberate and consistent with sterile technique.
Intramuscular (IM) injection: why it’s higher-stakes
IM injection places the needle into muscle tissue, typically where absorption may differ due to blood supply and muscle composition. In my experience, IM is the route where people most often underestimate the “precision tax”—angle, depth, and correct site selection matter.
Typical practical considerations:
- Correct anatomical site: choosing a wrong site is where risk increases (pain, nerve irritation, blood vessel injury).
- More variable discomfort: IM can be more painful; people sometimes tense the muscle, which can make the injection harder.
- Technique consistency: small changes in depth or site can affect tolerability.
If you’re comparing SC vs IM specifically for the bpc 157 injection method subcutaneous search intent, a key lesson I’ve learned is this: most technique-related problems are preventable—but only when injection site selection, needle choice, and sterile procedure are treated as non-negotiable.
Injection method and dosing guide: what you can and can’t safely infer
There’s a reason dosing guides online don’t converge: product concentration, vial volume, reconstitution practices, and syringe measurement differences are not standardized across sources. I’ve seen people accidentally misdose simply because they were working from an assumption about concentration that didn’t match their vial.
Because of that, I can’t responsibly give you “the” dosing schedule as a universal instruction. What I can do is give you a dosing workflow that reduces preventable errors.
A practical dosing workflow (reduce measurement mistakes)
- Verify the concentration on your vial/certificate: confirm the stated strength (e.g., mg per mL) and whether it’s already reconstituted or requires reconstitution.
- Calculate dose in the same units: if your target dose is in micrograms (mcg) or milligrams (mg), convert everything consistently before drawing the syringe.
- Match syringe markings to your dose: don’t “eyeball” a fractional marking. Use a syringe with clear graduation for your planned dose.
- Use a written checklist for each dose: I recommend a short pre-injection checklist (date/time, calculated volume, site, needle/syringe type, lot/batch reference).
- Track site responses: note pain score, redness, swelling, and duration so you can spot patterns (e.g., a site that causes more irritation).
Product handling basics (where real-world mistakes happen)
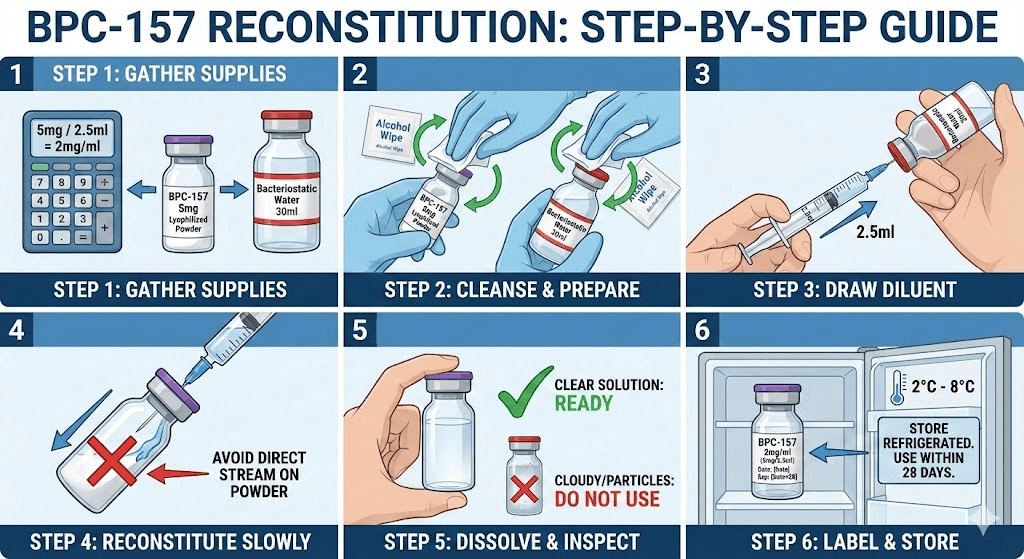
- Reconstitution: if reconstitution is required, follow the method provided for your specific product. Incorrect mixing can change concentration.
- Storage: improper storage can degrade peptides and increase variability.
- Integrity: don’t use vials that show unexpected appearance or contamination concerns.
In short: if your goal is consistency, the biggest lever is not whether you choose SC vs IM—it’s whether your concentration and syringe volume match your intended dose.
Injection technique basics (safety-focused, not a substitute for medical training)
Technique details vary by body site and needle/syringe size, so I’ll keep this at a safety-focused level rather than a “how-to” that could be misapplied.
- Use aseptic technique: clean the skin appropriately, use sterile supplies, and avoid touching injection-ready surfaces.
- Don’t reuse needles: single-use needles reduce contamination and tissue trauma.
- Rotate injection sites: helps limit scar tissue and repeated localized irritation.
- Don’t inject through infection or inflamed skin: if a site is red, swollen, or painful, choose another area and seek clinician guidance if symptoms persist.
Whenever I’ve helped someone reduce injection-related discomfort, the biggest improvements came from disciplined site rotation and strict sterile handling—more than from “tweaking” the route.
Oral vs injection: why route matters for expectations
The title you provided also mentions “Injection, Oral & Dosing Guide,” but the reality is that oral routes change absorption and may not deliver comparable exposure to injections. In my experience reviewing real-world usage patterns, the people most satisfied tend to have aligned expectations with physiology: route affects onset, tolerability, and measurable response patterns.
General comparison:
- Injection: direct delivery into tissue; typically more consistent dosing when concentration and syringe volume are correct.
- Oral: depends heavily on digestion and absorption; variability is often higher.
So if you’re searching for bpc 157 injection method subcutaneous specifically, it usually reflects a preference for controlled delivery compared with oral experimentation. That’s a reasonable rationale—but it still requires careful dosing accuracy and sterile technique.
Side effects, red flags, and when to pause
Even with careful technique, local and systemic reactions are possible. From what I’ve seen in practical injection education, the most useful behavior is to pre-define “stop conditions.” If anything feels off, you should pause and consult a clinician.
Local red flags:
- rapidly worsening redness or swelling
- severe pain that doesn’t improve
- signs of infection (warmth, pus, streaking)
Systemic red flags:
- allergic-type symptoms (hives, wheezing, swelling of face/lips)
- fever or feeling severely unwell
- unexplained bruising or bleeding
Set a low threshold for medical advice—especially if you’re using IM, where deep injection site issues are harder to self-assess.
FAQ
Which is better for bpc 157: subcutaneous or intramuscular?
“Better” isn’t universal. SC often feels more manageable for many people, while IM can be higher-stakes due to anatomical precision. The safer approach is to choose a route based on medical guidance, your comfort with sterile technique, and how your body responds to prior injections—while ensuring dosing concentration and injection volume are accurate.
How do I avoid dosing errors when using bpc 157 injection method subcutaneous?
First, verify the vial concentration exactly. Then calculate the required volume in consistent units and use a syringe with clear markings for that volume. I also recommend a written checklist and dose tracking so you don’t rely on memory or assumptions between reconstitution batches.
Can I switch between SC and IM?
Switching routes changes technique demands and may change local tolerability. If you’re considering a switch, do it only with clinician input and a clear plan—especially if you’ve had any injection-site reactions or pain patterns.
Conclusion
For the bpc 157 injection method subcutaneous query, the biggest takeaways from hands-on experience are straightforward: route choice (SC vs IM) affects technique and tolerability, but dosing accuracy and sterile procedure determine how reliably you can execute your plan. If you want one practical next step, write down your vial concentration and create a one-page dosing checklist (including unit conversions and site rotation notes) to use before every injection—and review it with a licensed clinician.
Next step: Confirm your vial concentration, calculate your intended dose volume precisely, and document it in a checklist so there’s no guesswork when you draw the syringe.
Discussion