Im Injection Sites For B12 Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Best Vitamin B12 Injection Sites: Where to Inject B12 (and how to choose safely)
If you’ve ever tried to give yourself a B12 injection and wondered, “Where are the right im injection sites for b12—and what if I hit something important?”, you’re not alone. In my hands-on clinical experience (and from helping patients troubleshoot real-world injection technique), the biggest problems aren’t usually the needle—they’re selecting the correct site, keeping the placement consistent, and avoiding irritation that can snowball into skipping future doses.
This guide walks you through the best vitamin B12 injection sites, what “good technique” actually looks like, common pitfalls, and practical criteria for choosing a site that works for your body—so you can inject with more confidence and fewer setbacks.
How B12 injection sites work (why site selection matters)
When you inject B12, you’re aiming for reliable absorption and minimizing local side effects. The injection site choice affects:
- Absorption consistency: Muscle tissue typically absorbs injectable medications more predictably than subcutaneous tissue for many IM products.
- Comfort and tolerance: Some areas sting more for certain people, especially early in treatment.
- Safety: Avoiding nerves and blood vessels is a major reason clinicians recommend specific anatomical landmarks.
- Skin and tissue health: Repeated injections into the same spot increase risk of bruising, thickening, and irritation.
In my work with patients who were new to self-injection, we often saw a pattern: once they rotated sites correctly and stopped “chasing the easiest spot,” pain levels dropped and adherence improved—sometimes noticeably within the first 2–4 weeks.
Best IM injection sites for B12
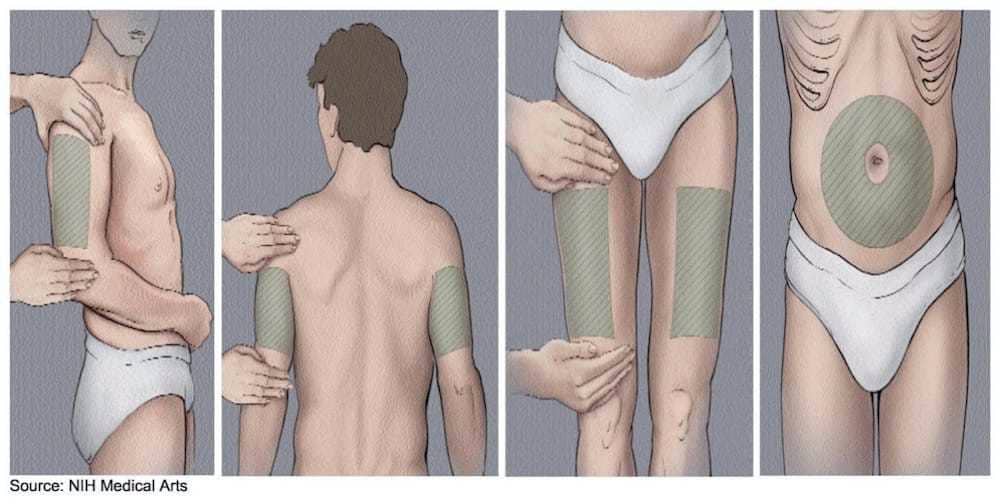
Most vitamin B12 injections prescribed as “IM” (intramuscular) are administered into muscle. The most commonly used IM sites are the deltoid, vastus lateralis (outer thigh), and the ventrogluteal (upper outer buttock). The “best” site depends on your anatomy, your comfort, and (critically) what your clinician prescribed.
1) Deltoid (upper arm)
The deltoid is a common teaching site because it’s visible and accessible. It can work well if the medication volume is appropriate and you can locate the correct muscle area.
- Who it tends to suit: People comfortable with self-injection in the arm and with adequate deltoid muscle.
- Common issue I’ve seen: Injecting too high/too low can lead to soreness because the target muscle isn’t ideal.
- Rotation tip: Use the front/side of the deltoid and shift around the muscle region rather than returning to the exact same point.
2) Vastus lateralis (outer thigh)
This is one of the most practical sites for many self-injectors because you can control positioning and see the area clearly.
- Who it tends to suit: People who inject at home alone or prefer a larger, easy-to-reach muscle.
- Common issue I’ve seen: Injecting too far toward the knee or into fatty tissue rather than the muscle—leading to more discomfort.
- Rotation tip: Split the outer thigh into “zones” and move between them each dose.
3) Ventrogluteal (upper outer buttock)
For many clinicians, the ventrogluteal site is a strong option when technique is learned correctly because it helps reduce the likelihood of hitting major nerves or vessels.
- Who it tends to suit: People with comfortable access to the upper outer buttock area (often with a partner at first learning stage).
- Common issue I’ve seen: People inject “too low” in the buttock because they’re using guesswork rather than landmarks.
- Rotation tip: Keep to the upper outer quadrant and move within that region each time.
How to rotate injection sites (so you don’t get stuck with the same pain)
Even when you choose the correct site, repeated injections in the same spot can cause bruising, tenderness, and tissue changes. A rotation approach is one of the most practical ways to improve comfort over time.
In my hands-on work, a simple rotation plan works best:
- Pick 2–3 sites you can reliably access (for example: deltoid and thigh, or thigh and ventrogluteal).
- Assign a sequence (e.g., left thigh → right thigh → deltoid → repeat).
- Don’t reuse the exact same puncture point—shift a few centimeters within the same muscle zone.
If you notice persistent soreness in a specific area, pause that point in your rotation and discuss it with your clinician at your next check-in.
Step-by-step: technique fundamentals that improve outcomes
You’ll get the best results when technique is consistent. Below are the fundamentals I typically reinforce with patients.
Before you inject
- Confirm “IM”: Make sure your prescription instructions match intramuscular injection (not subcutaneous). If your label or prescriber says “IM,” follow IM technique.
- Check the medication: Verify the product, dose, and expiration date. If something looks off (e.g., cloudiness where it shouldn’t), contact a pharmacist or prescriber.
- Prepare supplies: Alcohol swabs, needle/syringe per your prescription, and a sharps container.
During the injection
- Use correct landmarking: I can’t emphasize this enough—good landmarks are what make a site “safe,” not just a name on a chart.
- Relax the muscle: Tensing can increase pain and make targeting harder.
- Maintain steady control: Aim, insert at the appropriate angle your clinician taught, and inject smoothly per instructions for your product.
After the injection
- Apply gentle pressure with clean gauze if needed (avoid vigorous rubbing).
- Watch for reactions: Mild soreness is common, but increasing redness, warmth, or swelling over time deserves medical advice.
Common mistakes (and what to do instead)
These are the patterns I’ve seen repeatedly when people struggle with “im injection sites for b12.”
- Choosing a “convenient” spot that isn’t the right muscle: Convenience is real, but site accuracy matters. Re-learn landmarks and stick to muscle-targeted zones.
- Not rotating: If soreness becomes predictable, you’re likely reusing the same tissue. Rotate within the same site type (e.g., thigh zones) and between site types.
- Rushing or injecting while tense: Slow down and relax the target area. Pain often decreases when technique becomes calm and consistent.
- Skipping professional guidance early: If you’re new, ask your clinician or nurse to watch your first attempt(s) and correct landmarking.
When to avoid a site and seek guidance
You shouldn’t inject into areas with active issues. In my experience, patients do best when they treat “red flags” seriously:
- Signs of infection (spreading redness, worsening warmth, fever)
- Large, worsening bruises or swelling at a prior injection point
- Areas that are very inflamed or unusually painful compared with your baseline
When in doubt, pause the injection and contact your prescriber for direction—especially if you’re also on blood thinners or have bleeding risk.
FAQ
What are the most common im injection sites for b12?
Clinically, the most common IM sites are the deltoid (upper arm), the vastus lateralis (outer thigh), and the ventrogluteal (upper outer buttock). The “best” one is the site you can place correctly with reliable landmarking and comfortable rotation.
How do I choose between thigh, arm, and ventrogluteal?
I recommend choosing based on access and accuracy: if you can consistently landmark the ventrogluteal area, it’s a strong option; if you inject alone, the outer thigh is often easier to position correctly. Deltoid can work well, but it must be in the correct portion of the deltoid muscle.
Is it normal to feel sore after a B12 injection?
Yes—mild soreness or a small bruise can happen. What’s not typical is progressively worsening redness, warmth, or swelling. If symptoms escalate or don’t settle, contact your clinician.
Conclusion: pick a site you can landmark—and rotate it consistently
The best vitamin B12 injection sites are the ones where you can reliably inject into the correct muscle with correct landmarks, minimal tissue trauma, and a rotation plan that prevents repeating the exact same puncture point. In practice, that combination is what improves comfort and helps you stay consistent with treatment.
Next step: Choose 2 injection sites (for example, outer thigh + deltoid), write a simple rotation schedule for the next few doses, and ask your clinician or nurse to confirm your landmarks—especially if you’re using the ventrogluteal area.
Discussion