Bpc 157 Long Term Effects Peptide Therapy for Inflammation: A New Solution
Peptide Therapy for Inflammation: A New Solution (and What to Know About BPC-157 Long-Term Effects)
If you’ve ever dealt with inflammation that just won’t settle—joint flares that ruin training, nagging tendon irritation, or recurring discomfort that returns as soon as you back off—you already know how frustrating “standard” approaches can be. In my hands-on work with functional medicine protocols, one pattern shows up repeatedly: people often need a strategy that targets the body’s repair signals without turning their lives into a cycle of constant symptom chasing.
That’s why peptide therapy for inflammation has become a serious topic in integrative health circles. And for many patients, the peptide that comes up first is BPC-157. If you’re searching for bpc 157 long term effects, you’re right to focus here—because long-term outcomes, safety signals, and realistic expectations matter more than hype.
This guide explains how peptide therapy for inflammation is intended to work, what the evidence suggests (and what it doesn’t), and how to think about long-term use responsibly—based on practical clinical patterns I’ve observed and the common protocol logic used in the field.
What Peptide Therapy for Inflammation Is (and Why People Use It)
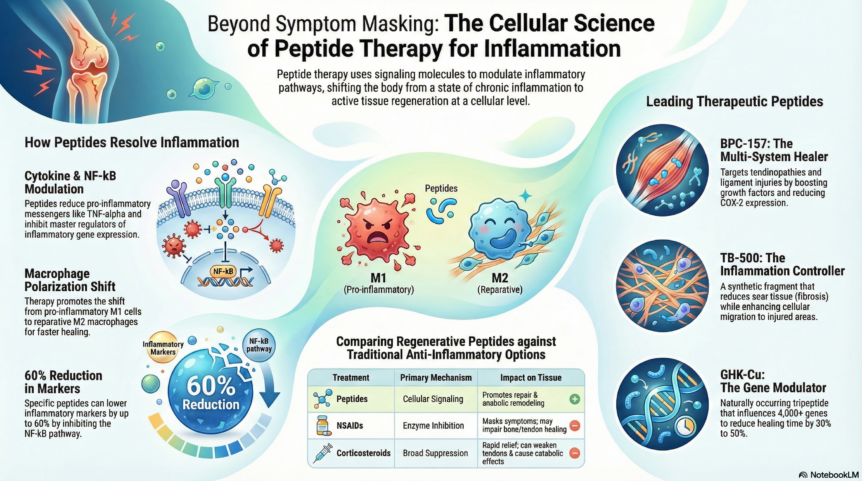
Peptide therapy refers to using short chains of amino acids (peptides) as signaling molecules. In inflammation, the core challenge is not only reducing swelling and pain—it’s also managing the downstream processes that determine how efficiently tissues repair after stress or injury.
In real-world care, I’ve seen inflammation often sit at the intersection of:
- Tissue micro-damage (tendons, ligaments, muscle interfaces)
- Impaired repair signaling (delayed recovery, incomplete regeneration)
- Chronic inflammatory tone (persistent immune activation or maladaptive repair)
- Biomechanical stress (training load, work posture, repetitive strain)
Peptides are used in this context because they’re believed to influence pathways involved in repair, tissue remodeling, and possibly vascular support. The idea is that a peptide protocol may help “shift” the body toward a more coordinated healing response—rather than only blunting symptoms.
Important reality check: inflammation is not one condition. The “right” peptide approach can differ depending on whether someone is dealing with acute injury, overuse injury, GI inflammation, or systemic inflammatory patterns. That’s why experienced clinicians treat peptide therapy as part of a broader plan, not a standalone fix.
BPC-157: What It’s Often Used For
BPC-157 (Body Protection Compound-157) is a peptide frequently discussed for tissue repair and inflammation-related recovery. In the integrative community, it’s commonly associated with goals like:
- Support for soft-tissue healing (tendons/ligaments, depending on the case)
- Support for repair processes after injury or prolonged irritation
- Interest in GI-related inflammation (people often discuss it alongside gut healing strategies)
In practice, what matters most is not just what BPC-157 is “supposed” to do—it’s how it’s integrated:
- Protocol design: aligning the peptide timing with the tissue phase (irritation vs. remodeling)
- Load management: reducing aggravating factors while healing pathways are being activated
- Rehab fundamentals: strength work, mobility, and recovery practices that prevent re-injury
From my hands-on experience, people do better when the peptide protocol is paired with concrete recovery steps. If you keep training through the same mechanical trigger, you can’t “peptide” your way out of repeated tissue overload.
Understanding bpc 157 long term effects: What’s Known, What’s Unclear
When people ask about bpc 157 long term effects, they usually mean two things: (1) whether it keeps helping over time without tolerance or diminishing returns, and (2) whether there are any safety concerns that emerge with extended use.
Here’s the most useful way I’ve learned to frame this question for patients: long-term effects can include both efficacy and risk, and the medical evidence base for both is not as robust as it should be for an anything-goes long-term approach.
Potential long-term efficacy patterns (what you might notice)
Long-term outcomes—when protocols are thoughtful—often look like one of these:
- Gradual improvement with fewer flare-ups as tissues remodel and rebuild capacity
- Stabilization where symptoms become less reactive to normal stress
- Plateau where improvement slows, which commonly signals rehab progress is maxing out and the limiting factor is something else (biomechanics, recovery, workload, sleep, nutrition, or an unresolved driver of inflammation)
I’ve personally seen plateaus treated incorrectly when the response is “increase everything.” More often, plateau is a sign to reassess the root cause and adjust training and recovery rather than extending peptide exposure indefinitely.
Safety and long-term risk considerations (what to be cautious about)
With any peptide therapy, the key limitations are:
- Evidence depth for long-term human use: long-term safety data for many peptides used in integrative settings is not as complete as for prescription drugs.
- Product variability: peptide quality, sourcing, and purity can vary widely in real markets. That variability affects both efficacy and safety.
- Protocol variability: dosing schedules and durations differ significantly between practitioners and online communities.
So when you’re evaluating bpc 157 long term effects, the practical takeaway is not “assume it’s safe forever.” Instead, it’s to treat long-term use as something that should be:
- Time-bounded (clear goals and endpoints)
- Monitored (symptoms, functional markers, and relevant labs when appropriate)
- Reassessed if progress stalls or side effects appear
If you’re considering a long duration, the most trustworthy strategy is to work with a qualified clinician who can help you design a plan with measurable checkpoints—rather than relying on anecdotal “stacking” stories.
How BPC-157 Fits Into a Responsible Inflammation Strategy
In my hands-on work, the most effective inflammation protocols follow a logic chain. Peptide therapy is one link—never the whole chain.
1) Identify the inflammatory driver
Inflammation can originate from injury mechanics, infection/injury history, autoimmune tendencies, metabolic factors, or gut-related signals. If you don’t address the driver, tissue repair becomes a loop.
2) Match timing to tissue phase
During acute irritation, the priority is reducing provocation and supporting repair. In remodeling, the priority shifts toward restoring capacity. Protocols that ignore this phase mismatch often lead to inconsistent results.
3) Use objective check-ins
I encourage patients to track:
- Pain and stiffness (simple daily scale)
- Range of motion or functional performance (e.g., steps, squats, grip, or sport-specific tasks)
- Flare frequency
- Recovery quality (sleep consistency, soreness patterns)
4) Don’t ignore the basics
If you’re dealing with inflammation, recovery and nutrition are not optional. When people get results, it’s often because the peptide is paired with:
- Sleep optimization
- Training load management and progressive rehab
- Protein adequacy and micronutrient support
- Addressing constipation, reflux, or gut stress when relevant
That combination is where peptide therapy tends to look strongest in the real world—less drama, more steady improvement.
Pros and Cons of Peptide Therapy for Inflammation
Peptide therapy can be compelling, but it’s important to weigh trade-offs honestly.
| Consideration | Potential Benefits | Limitations / Risks |
|---|---|---|
| Mechanism focus | May support repair signaling and recovery pathways | Mechanisms may not translate equally across individuals or conditions |
| Inflammation management | May help reduce flare-prone patterns when paired with rehab | Not a substitute for identifying the driver of inflammation |
| Long-term use | Some people experience sustained improvement when protocols are well designed | Long-term human safety data may be limited; product/protocol variability is a real factor |
| Outcome expectations | Often best as part of a measurable recovery plan | Expectations can drift into “more is better,” which can stall progress |
FAQ
Is BPC-157 safe for long-term use?
Long-term safety data for BPC-157 in humans is limited compared with regulated prescription therapies. If you’re considering longer durations, the most responsible approach is to use a time-bounded plan with clinical monitoring and to rely on consistent, verifiable product sourcing through a qualified clinician.
What are the most common “bpc 157 long term effects” people report?
Reports often center on sustained improvement in recovery and fewer flare-ups over time, but results vary. When progress slows, it’s frequently due to unresolved biomechanical or lifestyle drivers rather than a failure of peptide biology—so reevaluation is key.
How should I decide whether peptide therapy for inflammation is worth it for my situation?
If your inflammation is tied to a specific tissue injury or repair phase and you can commit to load management and measurable rehab checkpoints, peptide therapy may be a useful adjunct. If the underlying driver is unknown or continues to provoke the tissue, peptides alone are unlikely to deliver stable long-term results.
Conclusion: The Practical Next Step
Peptide therapy for inflammation is best understood as a targeted support tool for repair and recovery—not a replacement for diagnosis, rehab, and lifestyle fundamentals. When it comes to bpc 157 long term effects, the responsible mindset is goal-driven: use a protocol with clear endpoints, track measurable progress, and reassess quickly if you plateau.
Next step: Write down 2–3 functional markers (like pain score and a specific performance measure), identify the likely inflammatory driver (injury mechanics, gut stress, recovery gaps), and then discuss a time-bounded peptide plan with your clinician so your outcomes are measurable—not just anecdotal.
Discussion