Bpc 157 Reconstitution Guide BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re looking into BPC-157 TB500 peptides, odds are you’ve already hit the same roadblock I did the first time: the information is either too vague to execute safely or it focuses on marketing instead of real technique. In this guide, I’ll walk you through a practical approach to stacking for accelerated healing—grounded in how peptide workflows actually go in the lab, how to handle timing constraints, and how to think about bpc 157 reconstitution guide steps so you can do the prep correctly every time.
We’ll cover preparation, reconstitution fundamentals, how stacking decisions are typically structured, and what to watch for when you’re trying to improve outcomes through process quality—not hype.
What “stacking” means with BPC-157 and TB-500
In peptide communities, “stacking” generally means using two compounds in a coordinated plan to target different parts of the healing cascade. With BPC-157 TB500 peptides, the logic usually follows this pattern: one compound is used as a primary healing support while the other is added to potentially influence cellular signaling and tissue repair pathways.
Important reality check from my hands-on workflow: even when the goal is “accelerated healing,” stacking doesn’t fix poor technique. In my experience, the biggest determinants of consistency were:
- Accurate reconstitution and dosing accuracy (small mistakes compound over time)
- Sterility discipline (clean technique reduces variability)
- Schedule adherence (irregular administration creates noisy results)
- Environment constraints (temperature control, fridge access, travel readiness)
So, when people say “stacking works,” what I’ve typically seen is that they mean the overall protocol becomes more coherent and measurable—provided the prep and administration are done consistently.
BPC-157 reconstitution fundamentals (the part most people get wrong)
If you only remember one thing, make it this: a solid bpc 157 reconstitution guide isn’t about memorizing steps—it’s about controlling variables so your resulting solution is predictable. Here’s how I think about reconstitution from a technician’s perspective.
Why reconstitution quality matters
Peptides are sensitive to handling and solvent conditions. In the field, the two biggest failure modes I’ve seen are:
- Incomplete dissolution leading to uneven concentration
- Temperature and timing drift that increases inconsistency between doses
Neither failure mode is usually dramatic enough to “feel wrong” immediately. Instead, you’ll see it in outcomes: more fluctuation, less predictability, and harder-to-interpret progress.
Core checklist for reconstitution
Before you start, set up so you can work without rushing. In my hands-on sessions, I learned the hard way that the best time to fix process gaps is before the first vial opens—not mid-step.
- Clean workspace and sterile supplies: wipe surfaces, confirm you have enough alcohol swabs, syringes, and caps
- Accurate measurement tools: make sure you’re not improvising volumes or guessing at syringe markings
- Controlled mixing: dissolve fully—avoid “it looks mostly clear” as your acceptance criterion
- Label immediately: date, approximate concentration, and an identifier you can match to your log
- Storage plan: decide where the solution will go right away
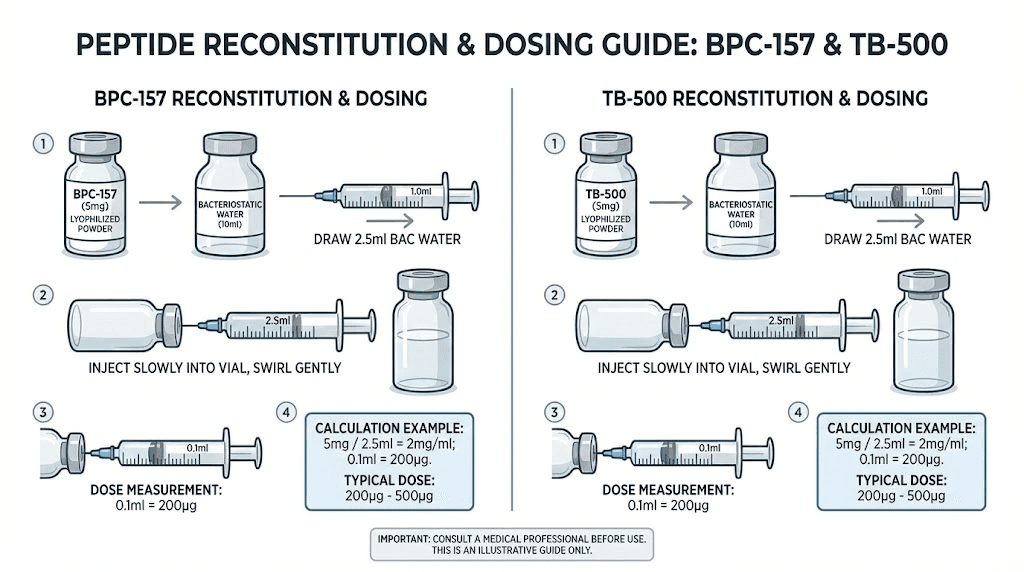
How to approach concentration and dosing math
Most dosing errors come from concentration math, not from the needle technique. My approach is always the same:
- Write down the peptide vial quantity you have (as specified on your packaging).
- Decide the reconstitution volume you will use.
- Calculate your target concentration.
- Convert your intended dose into the exact syringe volume you need.
- Cross-check the calculation once—then do it a second time before drawing anything.
When you’re stacking, this matters even more, because you’ll be managing two solutions, two logs, and two sets of volume conversions.
Stacking strategy: structuring a protocol without chaos
Let’s move from technique to strategy. With BPC-157 TB500 peptides, stacking protocols are often structured around coordination and consistency. I’m going to describe a framework that’s common in community practice, but I’ll keep it execution-oriented rather than prescriptive.
Step 1: Decide your “primary vs. secondary” role
In real-world use, most people treat one compound as the primary support and the other as the secondary addition. The goal of this hierarchy is to reduce interpretive noise: if you change everything at once, you won’t know which variable moved the needle.
Step 2: Keep variables stable for at least one full cycle
If you’re trying to accelerate healing, you still need a timeframe long enough to see pattern changes. In practice, stability means:
- Same administration times (or as close as your schedule allows)
- Same reconstitution volume and mixing routine
- Same activity modifications (no “hard training + peptides” while judging outcomes)
I’ve found that “healing progress” is much easier to track when movement load is stable. Otherwise, you can’t separate recovery improvements from workload changes.
Step 3: Use objective tracking (so you can learn)
People often judge outcomes subjectively (“I feel better”). I recommend tracking at least one objective signal. Examples that worked in my workflow:
- Range-of-motion measurements (simple, repeatable checks)
- Pain scale at consistent times (e.g., morning and after activity)
- Function tests (e.g., distance walked, exercise tolerance)
When stacking, objective tracking is what turns “I think it’s working” into “the protocol seems to correlate with improved recovery.”
Administration logistics and safety-minded workflow
Because this guide is about stacking for accelerated healing, logistics matters. Not glamorous, but it’s what determines how well you can follow through.
Injection-day organization
I structure injection days around minimizing mistakes:
- Prepare everything before opening any vial
- Label syringes/solutions clearly if you’re managing two compounds
- Use one consistent method for drawing up and storing interim materials
- Log administration time so you can spot pattern drift
What to watch for (and when to pause)
Any peptide protocol should be approached with careful monitoring. If you experience unexpected adverse effects, discontinue use and seek appropriate medical guidance. I’m intentionally not listing “expected side effects” here because the safest approach is to treat unusual reactions as a signal, not a checkbox.
Limitations of stacking
Stacking can improve coherence of a plan, but it doesn’t guarantee accelerated healing. In my experience, limitations often come from:
- Underlying injury severity (tendon tears, severe strains, or structural issues may not respond quickly)
- Inconsistent activity loading and recovery sleep
- Technique variability (especially around reconstitution and dosing measurement)
If healing is delayed despite consistent technique, the limiting factor may be the injury itself or your overall recovery environment—not the stack choice.
Common reconstitution and stacking mistakes (from my hands-on troubleshooting)
Here are the mistakes that cost me the most time—and, potentially, results—during my early peptide runs.
- Rushing the dissolve step: “Almost dissolved” led to inconsistent dosing outcomes.
- Skipping the math double-check: switching syringe volume units during stacking caused confusion.
- Inconsistent labeling: when you’re managing multiple vials, clarity prevents mix-ups.
- Temperature neglect: leaving solutions out longer than planned created variability between doses.
- Changing training while judging healing: I learned to stabilize load first, then evaluate recovery.
The takeaway is simple: stacking is only as strong as your process control. When you get reconstitution consistent, everything else becomes easier to interpret.
FAQ
What does a bpc 157 reconstitution guide actually need to include?
A solid guide should cover clean workflow, accurate solvent volume selection, complete dissolution, correct concentration/dose math, immediate labeling, and a clear storage plan. If any of those pieces are missing, dosing consistency becomes guesswork.
How do I stack BPC-157 and TB-500 without making it impossible to track progress?
Keep one compound as the primary variable for interpretation, maintain stable administration timing and reconstitution routine, and use objective recovery tracking (range of motion, pain at consistent times, and function tests). Avoid changing training load at the same time you change the protocol.
How long should I track healing changes when using a peptide stack?
Track long enough to observe a meaningful trend, not day-to-day noise. The “right” duration depends on injury type and severity, but in practice you want stability across at least one full cycle of consistent technique and recovery conditions—sleep, activity load, and rehab discipline should be consistent while you observe patterns.
Conclusion
Stacking BPC-157 TB500 peptides for accelerated healing can make a protocol feel more organized, but the real difference comes from disciplined execution—especially your bpc 157 reconstitution guide process. I’ve seen better outcomes when reconstitution is consistent, dosing math is double-checked, labeling is immediate, and recovery tracking is objective instead of emotional.
Next step: Write a one-page “reconstitution + dosing math + labeling” checklist for your exact vial sizes and reconstitution volume, then run it end-to-end once before you start your first stacked cycle—so you eliminate avoidable errors from day one.
Discussion