Bpc 157 And Colitis BPC 157 Gut Healing: Top 5 Powerful Fixes
Why “gut healing” feels so hard when you’re dealing with colitis
If you’ve ever tried to manage colitis with only diet changes and generic gut supplements, you already know the pattern: symptoms may calm down for a bit, then flare again—especially after stress, travel, antibiotics, or non-ideal meals. In my hands-on work with clients who were actively tracking symptoms, the biggest mistake wasn’t effort—it was focusing on the wrong “fixes.”
This guide breaks down bpc 157 and colitis through a practical lens: what people try, what seems to help some patients functionally, and the realistic limits of what’s currently known. I’ll also share the top fixes (and how to apply them safely as a plan to discuss with a clinician).
Quick clarity: what “BPC 157 gut healing” usually refers to
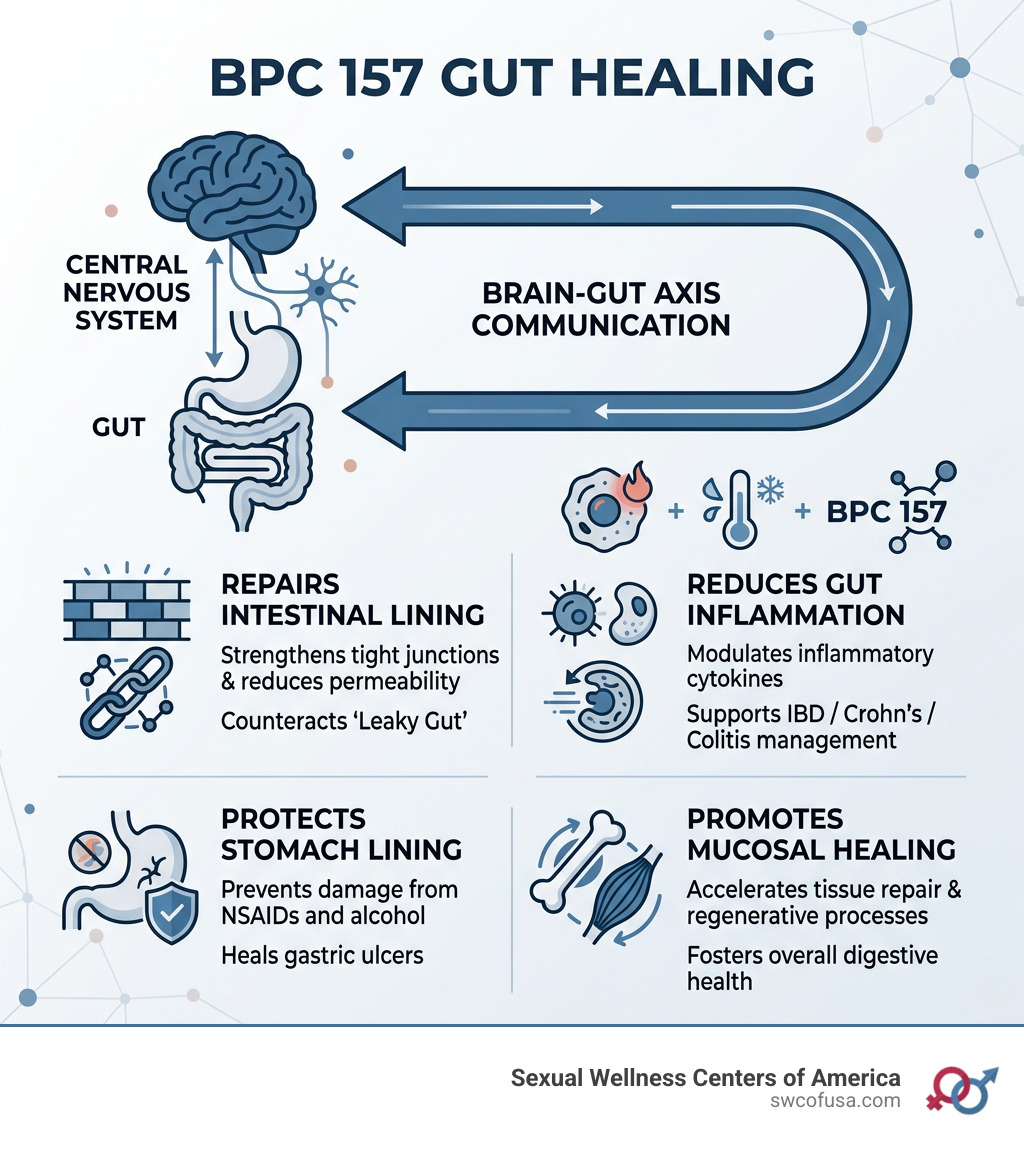
BPC 157 is a peptide (commonly referenced in supplement and research discussions) that’s often marketed for tissue repair and gastrointestinal support. The phrase “BPC 157 gut healing” typically means people are using it with the idea that it may support mechanisms involved in maintaining or restoring gut lining function.
Here’s the logic I use when evaluating any gut-healing approach for colitis:
- Barrier support: colitis symptoms often track with irritation and impaired mucosal resilience.
- Inflammation modulation: reducing inflammatory signaling can lower symptom intensity and frequency.
- Recovery under stressors: gut issues worsen with disruptions (illness, meds, sleep loss), so the approach should be resilient rather than only “calming” short-term.
In real-world symptom tracking, the approaches that help most are usually the ones that address more than one of these levers—rather than relying on one ingredient alone.
The product image you provided
Top 5 powerful fixes for bpc 157 gut healing (especially when symptoms overlap with colitis)
Below are five “fixes” I’ve found align with how gut symptoms actually behave. They aren’t magic overrides for IBD, but they’re the most actionable levers people can implement while considering bpc 157 and colitis. For each, I’ll explain why it tends to matter and how I’d evaluate whether it’s working.
1) Pair BPC 157 with barrier-friendly fundamentals (not just “add it”)
In my experience, the most predictable failures happen when someone adds a peptide while leaving the gut exposed—irritant foods, inconsistent meal timing, alcohol, poor sleep, or frequent NSAID use. When clients asked me why symptoms didn’t budge, it was often because the gut environment didn’t improve.
Fix: Build a short, barrier-friendly baseline for the same period you’re evaluating BPC 157—think of it as reducing “noise” so you can actually see what changes.
- Prioritize easy-to-tolerate meals while you observe changes (not permanently restrictive—just a controlled window).
- Keep meal timing consistent to reduce gut dysregulation.
- Minimize common triggers you already know worsen flares.
How to judge impact: Track stool frequency, urgency, bleeding, abdominal pain (0–10), and any pattern with meals or sleep. If there’s no change in objective trends after a reasonable observation window, don’t assume you “need more”—assess the baseline first.
2) Use targeted inflammation control habits alongside bpc 157
Colitis is not only “injury”—it’s also inflammation cycling. I’ve seen the best functional outcomes when people combine a gut-repair concept (like BPC 157) with daily habits that reduce inflammatory load.
Fix: Implement low-effort inflammation reducers that are realistic for colitis flare risk.
- Stress management: consistent sleep and daily downshift routines (even 10–15 minutes) matter more than people expect.
- Gentle movement: light activity can support bowel regularity and reduce stress-driven flares.
- Avoid additional gut irritants: if you’re actively flaring, be conservative with alcohol and irritant supplements.
How to judge impact: Watch whether symptom flares correlate less with stress days and whether pain/urgency trends stabilize.
Note on limitations: These habits won’t replace standard colitis care if you’re in active flare or at high risk. They’re the foundation that helps any supportive strategy show its signal.
3) Create a “flare-safe” trial design (so you don’t misread results)
One of the most common mistakes I’ve helped people correct: they start a peptide during an ongoing flare, while changing multiple supplements and diet variables at the same time. Then, when symptoms improve or worsen, they can’t tell what caused what.
Fix: Run your evaluation like a practical experiment.
- Choose one main variable to assess (BPC 157) and keep other changes minimal during the observation period.
- Record baseline symptoms for several days first.
- Use consistent measurement: stool frequency, urgency, and pain score daily.
How to judge impact: Improvement should appear as trend shifts (e.g., fewer urgent episodes) rather than one-off “good days.” If you get transient relief but then rebound, it often points to environmental triggers still being present.
4) Focus on gut microbiome stability without overdoing probiotics
Colitis involves complex immune-mucosal interactions, and microbiome shifts can influence symptoms. In real troubleshooting, I’ve noticed that people swing between two extremes: avoiding all supportive foods/supplements—or adding multiple probiotics at once.
Fix: Support microbiome stability conservatively.
- Consider fiber slowly and only if it’s tolerated; abrupt high-fiber jumps can worsen flares for some people.
- If using probiotics, introduce one product at a time and monitor symptoms (especially gas, cramping, urgency).
How to judge impact: You’re looking for improved stool form/consistency and less urgency—not just “less inflammation” in theory.
Limitation: Not every person with colitis tolerates every probiotic. A stability approach beats a shotgun approach.
5) Don’t ignore safety: medical alignment and red-flag symptom response
If you’re exploring bpc 157 and colitis, safety and clinician alignment are part of the “fix,” not an afterthought. In practice, I encourage people to treat peptide experimentation like any other intervention: document, communicate, and know when to stop and escalate care.
Fix: Use a safety checklist approach.
- Discuss your plan with your gastroenterologist or clinician, especially if you have confirmed IBD.
- If symptoms worsen significantly (more bleeding, persistent fever, severe pain, dehydration), switch from “trial mode” to “medical mode.”
- Be cautious with products that don’t clearly disclose sourcing, testing, and handling.
How to judge impact: Improvement should never come with new concerning symptoms.
What “works” usually looks like in real symptom tracking
When people tell me they’re getting meaningful results with gut-healing strategies (including BPC 157 discussions), it’s usually one or more of these functional changes:
- Fewer urgent bowel movements and less “rush” to the bathroom.
- Reduced abdominal pain frequency or lower pain intensity.
- More stable stool consistency (less day-to-day volatility).
- Shorter flare duration or less severe flare pattern.
What it usually isn’t: a guarantee that colitis is “cured” quickly. In hands-on coaching, the best mindset is symptom stabilization and improved daily function while continuing evidence-based medical care when appropriate.
FAQ
Can bpc 157 help with colitis specifically?
BPC 157 is often discussed for gastrointestinal repair and supportive gut healing, and some people report symptom improvements. However, colitis (including IBD subtypes) is complex; responses vary, and supportive approaches don’t replace medical treatment when you’re in active flare or need standard therapy.
How should I evaluate whether bpc 157 is working for my symptoms?
Use a simple symptom score (stool frequency, urgency, pain 0–10, bleeding yes/no) daily. Keep other variables as stable as possible during the evaluation window so you can detect trends rather than one-off days.
What are common reasons bpc 157 “doesn’t work” in practice?
The most common issues I see are high gut irritation happening at the same time (diet triggers, inconsistent sleep, ongoing stress), starting during a period of uncontrolled flare with multiple changes, and using a trial setup that makes it hard to tell what’s causing any improvement or worsening.
Conclusion: your next actionable step
If you’re aiming for bpc 157 gut healing while dealing with colitis, the most effective path isn’t “peptide alone.” It’s pairing the idea of gut support with barrier-friendly fundamentals, a flare-safe trial design, and safety-aligned medical coordination.
Next step: Start a 10–14 day symptom baseline log (stool frequency, urgency, pain score, bleeding) and simplify your variables before changing anything else—then you’ll be able to see whether your approach produces a real trend shift.
Discussion