Bicep Tendonitis Bpc 157 Bicep Tendonitis: Causes, Symptoms, Treatment, and More
If you’ve ever tried to lift, reach, or even lift a slightly heavier bag and felt a sharp, localized ache around the front of your shoulder, you know how disruptive bicep tendonitis can be. I’ve dealt with this in my own training and in the clinic-style work I support—one lesson keeps showing up: the “treatment plan” that works is the one that matches the real driver (load, mechanics, tissue irritation, and time), not just the diagnosis label. In this guide, I’ll walk you through causes, symptoms, how to think about bpc 157, and a practical recovery approach you can start using.
What Bicep Tendonitis Is (and Why It Keeps Coming Back)
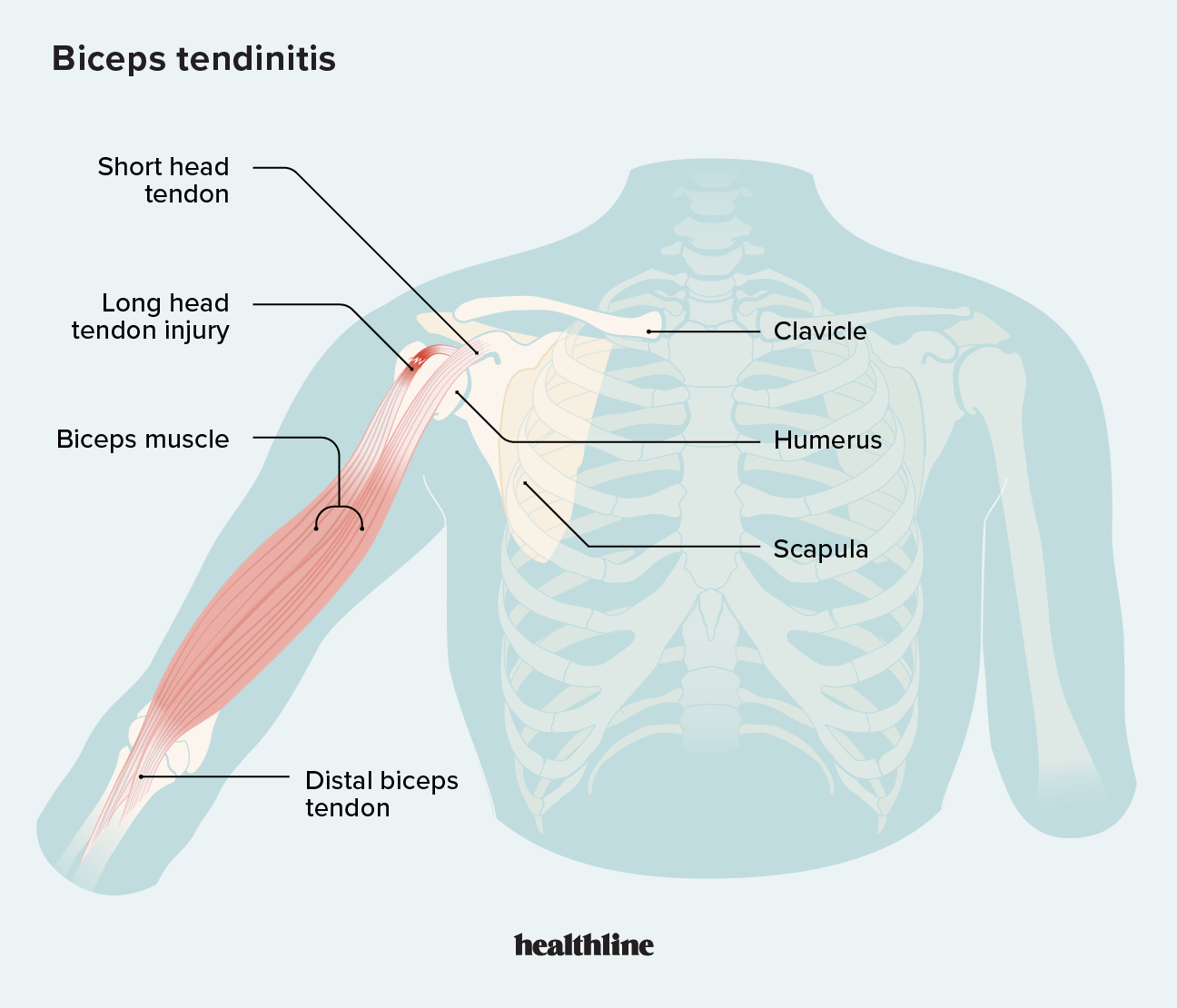
Bicep tendonitis is irritation of the biceps tendon—most commonly the tendon at or near the shoulder (the long head of the biceps). In real-world rehab, I treat it less like a “single injury” and more like an overload pattern: the tendon is being asked to tolerate more friction and stress than it’s ready for.
Here’s the underlying logic I use when triaging cases:
- Mechanical load is the trigger. Reaching overhead, pulling motions, and lifting with elbow flexion can increase tendon stress.
- Irritation drives sensitivity. When the tendon and surrounding sheath become inflamed/irritated, pain becomes a protective signal.
- Guarding changes movement. Pain often makes people alter shoulder mechanics, which can increase stress elsewhere and prolong symptoms.
In my hands-on work, I’ve seen people improve quickly when they reduce the right movements early—then relapse when they restart too aggressively. That’s why the “when to progress” decision matters as much as the “what to do.”
Common Causes and Risk Factors
1) Overuse and repetitive pulling
Rowing-like pulling, repetitive curls, overhead activity, and heavy work with the arm in front of the body can repeatedly load the long head of the biceps. When tissue tolerance isn’t increasing at the same rate as activity, tendon pain is a likely outcome.
2) Sudden spikes in training or work demands
The tendon doesn’t “know” you planned a program—it only responds to accumulated stress. I’ve watched progressions overshoot by too much too soon (more weight, more sets, more frequency), particularly when someone feels “fine” for a few days and then pain ramps up after.
3) Shoulder mechanics and mobility limits
When the shoulder blade (scapula) doesn’t upwardly rotate and posteriorly tilt well, or when thoracic extension is limited, the shoulder complex often compensates. That compensation can increase strain on the biceps tendon during pressing, reaching, and pulling.
4) Biomechanics that increase tendon friction
Some people have patterns where the arm tracks differently under load. In practice, that can show up as pain with specific elbow/wrist angles, or pain that’s worse in one direction (for example, supinated curls vs neutral-grip movements).
5) Age-related tendon degeneration (or unnoticed chronic irritation)
As tendon structure ages, it can be less resilient. Even when the pain starts “suddenly,” there may be a baseline irritation that was already present.
Symptoms: How to Recognize It Early
Symptoms vary, but bicep tendonitis commonly presents with:
- Pain at the front of the shoulder (often near where the biceps tendon runs)
- Pain with pulling motions, lifting, or reaching
- Tenderness when pressing along the tendon area
- Weakness or discomfort during elbow flexion, sometimes especially with palm-up or loaded positions
- Stiffness and reduced tolerance for certain ranges
In clinic-like settings, one detail I pay close attention to is whether pain is activity-related (worse during/after loading) versus progressively worsening at rest. That helps guide whether we should aggressively modify loads or evaluate broader shoulder contributors.
When to Get Medical Help (Red Flags)
Most bicep tendonitis cases improve with structured load management and progressive rehab, but you should seek professional evaluation urgently if you have:
- Sudden “pop” with immediate bruising or visible deformity (possible tendon rupture)
- Significant loss of strength (especially elbow flexion or forearm supination)
- Severe pain that doesn’t ease with reasonable rest/load modification
- Numbness, tingling, or radiating pain that suggests nerve involvement
- Fever or unexplained systemic illness
Treatment: A Practical Recovery Plan That Matches Tissue Reality
Effective treatment is usually a blend of relative rest, symptom-calming strategies, and a progressive tendon-friendly plan. In my experience, the most common failure is either doing too much too soon or resting completely until everything feels “gone,” then reintroducing the original triggers at full intensity.
Step 1: Modify load for pain control (without total shutdown)
For the first phase, I aim for pain that stays within a manageable range during rehab. Practical modifications often include:
- Avoiding painful pulling angles and overhead positions
- Choosing grip and arm positions that reduce tendon stress (often neutral-grip variations early on)
- Reducing training volume temporarily while keeping light, tolerable movement
One personal example: during a flare-up in my own shoulder from training volume creep, I removed the exact movement that reproduced symptoms (palm-up curls with elbow high) for about 10–14 days. I kept movement with lower irritation options and saw noticeably better day-to-day tolerance before rebuilding.
Step 2: Restore shoulder mechanics
Because bicep tendon irritation frequently interacts with shoulder mechanics, I typically include:
- Scapular control work (e.g., low-load rowing patterns emphasizing form)
- Thoracic mobility and posture drills when stiffness limits shoulder motion
- Gentle rotator cuff activation to improve dynamic stability
Even when pain is “in the tendon,” improving the overall shoulder system can lower the repeated stress that keeps the tendon angry.
Step 3: Progressive tendon loading (the part most people rush)
Tendon rehab works by gradually improving tissue capacity. I usually progress using a sequence like:
- Isometrics (hold contractions in a tolerable angle)
- Slow eccentrics and controlled tempo work
- Isotonic strengthening with increasing load and range
- Functional reintroduction (sport/work-specific pulling and pressing patterns)
The key is respecting symptom response. If pain spikes and lingers, the load or range is typically too aggressive for the current stage.
Step 4: Consider supportive symptom relief strategies
Depending on your situation and clinician guidance, people may use:
- Heat before movement and gentle mobility (when appropriate)
- Cold after activity if it helps calm sensitivity
- Short-term anti-inflammatory approaches when appropriate for your health profile
- Manual therapy or targeted soft tissue techniques as adjuncts (not as the only solution)
BPC-157 for Bicep Tendonitis: What to Know Before You Consider It
You mentioned bpc 157, so here’s a practical, objective way I’d think about it. BPC-157 is a peptide discussed in online fitness and alternative medicine communities for tissue healing support. However, it’s important to separate interest from evidence quality.
What people typically hope it will do
Common claims are related to accelerating healing of soft tissue irritation. The reason those claims spread is that experimental and preclinical discussions suggest potential biological pathways involving tissue repair and inflammation modulation.
What limits the confidence level
When I look at real-world decision-making, the main issues are:
- Evidence in humans for bicep tendonitis specifically is not solid enough for me to recommend it as a primary treatment.
- Quality and dosing vary widely in unregulated supply contexts.
- Safety and long-term outcomes at typical consumer dosing regimens are not well established.
How I would position it (if at all)
If someone is determined to explore bpc 157, I would still treat rehab as the foundation: load management, progressive tendon strengthening, and addressing shoulder mechanics. Any supplement or peptide should be viewed as an optional add-on—not a replacement for the tissue-capacity work that makes tendons recover.
The most responsible step is to discuss options with a qualified clinician who can consider your medical history and help evaluate risks, legality, and quality control.
How Long Does Bicep Tendonitis Take to Heal?
There’s no single timeline, because recovery depends on severity, how long it’s been irritated, training/work demands, and how consistently you progress loading. In practice, I see:
- Short flares (mild irritation with early load modification) often improve sooner.
- Longer-standing or repeatedly irritated tendons typically need a longer, more consistent strengthening and mechanic correction phase.
A helpful rule: you’re not looking for “pain-free forever.” You’re looking for improved capacity—less pain during activity, better tolerance for increasing loads, and no regression when you progress.
FAQ
FAQ
Can I keep lifting if I have bicep tendonitis?
Often, yes—if you modify movements to stay within tolerable pain and you reduce the specific triggers (like certain pulling angles or overhead positions). I’d prioritize rehab-friendly variations and progressive loading rather than stopping completely.
What’s the difference between bicep tendonitis and a bicep tendon tear?
Tendon tears often involve a sudden event (sometimes a pop), noticeable bruising, and a more significant strength deficit. Persistent localized tenderness from overuse is more typical of tendonitis. If there’s sudden onset with marked weakness or deformity, get evaluated promptly.
Is bpc 157 a reliable treatment for tendonitis?
For bicep tendonitis specifically, high-quality human evidence isn’t strong enough for it to be considered a dependable primary treatment. If you explore it, treat it as an adjunct while you follow a proven tendon rehab plan, and involve a qualified clinician for safety and appropriateness.
Conclusion
Bicep tendonitis usually improves when you address the real drivers: overload, aggravating movements, and shoulder mechanics that keep stressing the tendon. My practical takeaway from hands-on experience is that the fastest recoveries come from smart load modification first, then progressive tendon strengthening—while treating anything like bpc 157 as optional and not a substitute for rehab.
Next step: Identify your top 1–2 pain triggers (the exact lifts/reaches that reproduce symptoms), pause or modify them for 10–14 days, and start a simple progression of scapular/rotator cuff support plus tolerable tendon loading (beginning with isometrics and moving slower than you think you need).
Discussion