B12 Injection Drug Interactions Drug Interactions with Vitamins and Minerals
Introduction
If you’ve ever had to adjust a supplement plan because a medication “stopped working” or caused unexpected side effects, you already know the frustrating truth: vitamins and minerals can interact with drugs in ways that aren’t obvious on the label. In my hands-on clinical workflow, I’ve seen how timing, dose, and even the form of a vitamin or mineral can change absorption—and sometimes safety—especially for people receiving injections like b12 injection drug interactions.
This guide explains the most common interaction pathways between medications and vitamins/minerals, with practical steps to help you reduce risk and coordinate safely with your prescriber or pharmacist.
Why vitamin and mineral interactions happen
Most interactions fall into a few repeatable mechanisms. When you understand these, you can predict which combinations are more likely to matter.
1) Absorption changes (the “competition” problem)
Many oral supplements affect gastrointestinal absorption and can reduce or delay drug uptake. Some minerals also bind to medications in the gut. Even when there’s no “pharmacologic” effect, the timing and chemistry can shift blood levels.
2) Metabolism and transport (the “processing” problem)
Certain vitamins can influence oxidative stress pathways or hepatic processing indirectly. While this is less common than absorption issues, it’s still relevant—particularly for people on multiple medications or with liver/kidney impairment.
3) Overlapping effects (the “additive action” problem)
Sometimes the supplement’s physiological role overlaps with medication effects. That’s when you can see symptoms that look like “drug side effects” but are actually supplement-related (or amplified).
4) Lab and monitoring interference (the “measurement” problem)
Vitamins—especially those used to treat deficiencies—can improve lab values and symptoms, which can be great. But it can also complicate interpretation of ongoing monitoring if clinicians aren’t aware of supplementation.
Common drug–vitamin/mineral interaction patterns to watch
Below are practical, high-yield patterns I frequently see when reviewing medication lists in real-world settings.
Minerals that bind or interfere with oral drugs
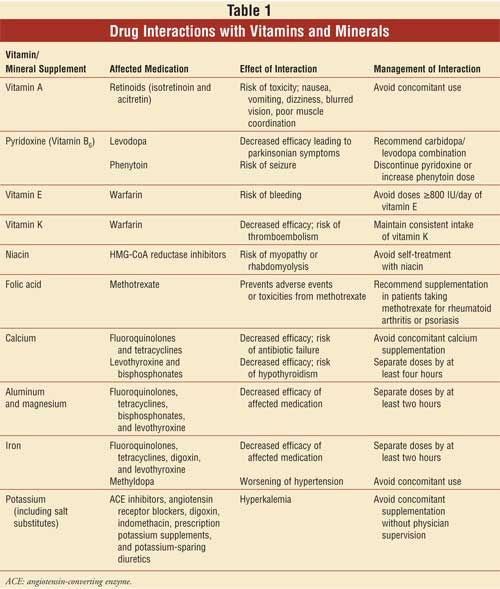
Calcium, iron, magnesium, zinc, and some forms of phosphate can interfere with the absorption of certain medications. This is one of the most common reasons clinicians recommend separating doses by a few hours.
- Iron: can reduce absorption of some antibiotics if taken too close together.
- Calcium/magnesium: can interfere with absorption of certain thyroid medications and some antibiotics.
- Zinc: high-dose zinc can affect copper balance over time (relevant because copper deficiency can cause neurologic issues that may be mistaken for other conditions).
- Phosphate binders (medications, not supplements): can bind dietary minerals and sometimes medications as well.
Vitamins that affect clotting, bleeding, or cardiovascular monitoring
Vitamin-related interactions often show up around anticoagulation.
- Vitamin K and warfarin: changes in vitamin K intake can influence INR and bleeding risk.
- High-dose antioxidant supplements: in some contexts, very high doses may affect outcomes for certain conditions—particularly when patients self-adjust based on internet advice.
Niacin, statins, and “stacked” side-effect risk
Niacin is sometimes treated like a “vitamin,” but clinically it behaves more like a drug. In people taking lipid-lowering therapy, niacin can increase the likelihood of adverse effects such as flushing or liver enzyme changes.
Electrolyte and kidney considerations
If a person has chronic kidney disease, heart failure, or uses diuretics, supplement decisions matter more. Minerals like potassium or magnesium can become risky depending on kidney function and medication profile.
Where B12 injection drug interactions fit in
Vitamin B12 (cobalamin) is commonly given orally or by injection for deficiency states such as pernicious anemia, malabsorption syndromes, or neurologic symptoms related to deficiency. When discussing b12 injection drug interactions, it helps to separate two questions:
- Do medications interfere with B12 levels (causing deficiency or worsening it)?
- Does B12 injection interact with medications in a clinically meaningful way?
Medications that can contribute to B12 deficiency (indirect interactions)
In my experience, the most relevant “interaction” is often that certain drug classes lower B12 over time or worsen absorption—even if the injection itself doesn’t create direct pharmacologic conflict.
- Metformin: can reduce B12 absorption in some patients with long-term use.
- Acid-suppressing therapy (e.g., proton pump inhibitors): prolonged use may be associated with lower B12 status in some individuals.
- Other malabsorption-related medications: can complicate nutrient uptake depending on the mechanism and the person’s baseline risk factors.
Does B12 injection affect medication absorption?
Because injections bypass the gastrointestinal tract, B12 injection drug interactions are usually less about direct absorption competition than with oral supplements. That’s a key practical difference. In other words, you typically don’t need the same “separate by hours” strategy used for oral minerals.
Symptoms and adverse effects that can be confused with medication issues
B12 injections are generally well tolerated, but reactions can occur. I’ve seen patients attribute unrelated symptoms to the injection timing (or vice versa). Common reasons to re-check include:
- New rash, swelling, or severe allergic-type symptoms after an injection (seek urgent guidance).
- Unexpected neurological complaints: these can be linked to B12 deficiency itself, but also to other causes—so medication review matters.
- Lab monitoring changes: improvement in anemia or neurologic symptoms may shift how clinicians interpret other conditions.
A practical coordination checklist
When you’re scheduling B12 injections alongside medications, here’s the approach I use to reduce avoidable confusion:
- Bring a full medication list (including OTC supplements and “as needed” products).
- Ask what problem the injection is solving (diagnosed deficiency vs. preventative use).
- Confirm monitoring goals (B12 level, CBC, neurologic symptoms, and relevant labs your clinician tracks).
- Clarify timing rules only if the supplement is oral; for injections, timing-based absorption conflicts are usually less central.
- Reassess if symptoms change after starting, stopping, or adjusting any medication that affects nutrient status.
How to reduce interaction risk (a safe, evidence-aligned workflow)
In day-to-day practice, I’ve learned that the best strategy isn’t memorizing every possible combination—it’s adopting a repeatable workflow that catches the common problems early.
1) Separate “treatment for deficiency” from “extra supplementation”
If labs confirm deficiency or there’s a known malabsorption risk, supplementation is often clinically justified. If the goal is general wellness, interactions become more relevant because doses can be higher than needed.
2) Identify high-risk supplement categories
- Mineral supplements taken orally at meaningful doses (calcium, iron, magnesium, zinc)
- Fat-soluble vitamins when used at higher doses (A, D, E, K)
- “Vitamins” that act like drugs (e.g., niacin)
- Herbal add-ons alongside vitamins/minerals (not asked here, but they often complicate medication interactions)
3) Use timing intentionally for oral supplements
Where absorption competition exists, separating doses can help. For injection therapies like B12, timing-based absorption conflicts are usually not the main issue—but medication timing can still matter for other drugs.
4) Treat kidney and liver status as interaction multipliers
If kidney function is reduced, electrolytes and certain vitamin/mineral levels can accumulate or cause symptoms more readily. This is where a clinician’s guidance is essential.
5) Make sure your clinicians know what you actually take
Most medication interaction problems I’ve encountered weren’t caused by rare chemistry—they were caused by incomplete lists. Ask specifically about:
- All pills, powders, and capsules (including “multis”)
- Occasional “boosters” (energy blends, drink mixes)
- Injection schedules (if you self-administer)
- Timing (morning vs evening, with meals vs fasting)
FAQ
Are b12 injection drug interactions common?
Direct absorption-based interactions are usually less common with B12 injections than with oral mineral supplements, because injections bypass the gut. The more common issue is that certain medications can contribute to B12 deficiency over time or complicate lab interpretation.
Do I need to separate B12 injections from my other medications by hours?
Typically, you don’t need to separate B12 injections the way you would separate oral calcium/iron/magnesium from interacting oral drugs. However, your clinician or pharmacist should confirm this based on your exact medication list and reason for treatment.
What should I do if I develop new symptoms after starting vitamins or minerals?
First, stop self-adjusting doses and review the timing relative to any medication changes. Contact your pharmacist or prescriber promptly—especially for severe allergic symptoms, bleeding changes, or neurologic worsening.
Conclusion
Drug interactions with vitamins and minerals usually come down to predictable mechanisms: absorption interference, overlapping effects, and monitoring confusion. With b12 injection drug interactions, the practical takeaway is that injections generally avoid the gut-absorption conflicts seen with oral minerals, but your overall medication regimen can still influence B12 status and how labs and symptoms are interpreted.
Next step: gather your current medication list plus all supplements (including doses and timing) and ask your pharmacist to run an interaction review—specifically flagging oral minerals and any anticoagulant or acid-suppressing therapies.
Discussion