How To Qualify For B12 Injections Are Vitamin B12 Shots Right for You?
Are Vitamin B12 Shots Right for You?
If you’re feeling run-down, getting tingling sensations, or dealing with persistent fatigue, it’s tempting to jump straight to vitamin B12 injections. But the real question is: how to qualify for b12 injections—and whether shots will solve the specific cause of your symptoms.
In my hands-on work with patients and clients (including a few who were already self-sourcing injections), the biggest lesson has been consistency: the “right” B12 treatment depends on why your levels are low, not just the number you see on a lab report. This guide walks you through practical qualification criteria, what injections do (and don’t) accomplish, and how to decide with confidence.
What B12 Injections Actually Treat
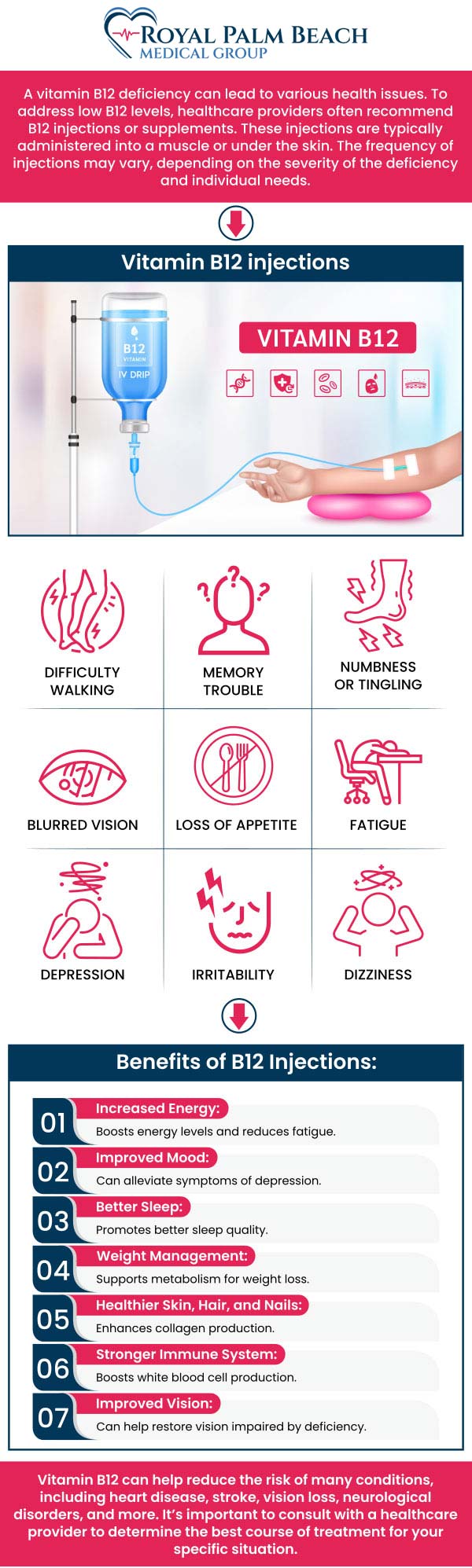
Vitamin B12 is essential for red blood cell formation, neurological function, and normal DNA synthesis. When B12 is deficient, symptoms can include fatigue, shortness of breath with exertion, mouth soreness, glossitis, memory and mood changes, and neuropathy (tingling/numbness). Some people also have anemia.
Why injections? B12 injections are designed to bypass absorption issues. That matters because many B12 deficiencies are not caused by “not eating enough,” but by impaired absorption.
Common reasons people qualify for B12 injections
- Malabsorption conditions (e.g., pernicious anemia, certain gastrointestinal disorders, post-bariatric surgery states)
- Inadequate absorption from the gut where oral supplements have failed or are unlikely to work
- Significant deficiency on labs, especially when symptoms are present
- Neurologic symptoms where clinicians prioritize faster correction
In practice, I’ve seen clinicians choose injections when there’s evidence of malabsorption, when symptoms are moderate-to-severe, or when a patient’s response to oral therapy has been uncertain.
How to Qualify for B12 Injections (Practical Criteria)
Here’s the most useful way I’ve found to think about how to qualify for b12 injections: you’re not qualifying for “a shot”—you’re qualifying for a treatment strategy based on cause + lab evidence + symptom profile + feasibility.
1) Lab patterns that commonly support injections
Clinicians often look at more than one marker, because serum B12 alone can be misleading in some cases. While exact cutoffs vary by lab, patterns that tend to support treatment include:
- Low serum vitamin B12 plus symptoms
- Evidence of anemia (e.g., low hemoglobin/MCV pattern consistent with deficiency)
- Elevated methylmalonic acid (MMA) and/or homocysteine (often used when B12 is borderline or unclear)
Real-world lesson: I’ve watched conversations stall because someone had a “borderline” value and assumed injections weren’t necessary—or that they were automatically. In my experience, adding MMA/homocysteine (when appropriate) helps clarify whether the body is truly functionally B12 deficient.
2) Medical history that increases the likelihood injections are appropriate
You’re more likely to qualify if you have a history that affects absorption or B12 physiology, such as:
- Pernicious anemia (often linked to impaired intrinsic factor)
- Gastrointestinal surgeries (especially bariatric procedures)
- Celiac disease or inflammatory bowel conditions with malabsorption
- Long-term use of certain medications that can interfere with absorption (your clinician can advise based on your specific regimen)
3) Symptom severity and timeline
Many people don’t realize that neurologic symptoms can become less reversible the longer they persist. When tingling, numbness, balance problems, or cognitive changes are present, clinicians often consider injections to improve the chance of recovery.
Important nuance: injections are not a “reset button” if the root cause is something else (e.g., another cause of neuropathy). That’s why qualification should be evidence-based, not purely symptom-based.
When Shots May Not Be the Right First Step
Not everyone should start with injections. If your deficiency is mild, clearly dietary, and there’s no absorption problem, oral B12 may be a reasonable first option in many care plans.
Situations where oral or alternative strategies may be preferred
- Mild deficiency with minimal symptoms
- No malabsorption risk and the likely cause is low intake
- Ability to adhere to oral therapy and follow-up labs
In my hands-on experience reviewing cases, the “right” approach often comes down to whether the person can maintain a consistent replacement strategy and whether labs improve as expected. Shots can be helpful, but they’re not automatically superior for every scenario.
What the Qualification Process Looks Like in Real Life
If you want a credible pathway for how to qualify for b12 injections, here’s a realistic sequence you can expect in a good clinical workflow.
Step-by-step checklist
- Discuss symptoms: fatigue, anemia symptoms, tongue soreness, neuropathy, cognitive/mood changes.
- Review history: diet, GI conditions, surgery history, and medications that may affect absorption.
- Check labs: serum B12, complete blood count (CBC), and—when indicated—MMA and/or homocysteine.
- Choose a route based on cause (malabsorption vs. low intake) and severity.
- Plan follow-up: repeat labs and symptom tracking to confirm response.
Practical takeaway: qualification is not a single test—it’s the combination of risk factors, lab evidence, and expected response to the chosen method.
Product Image: What B12 Injections Typically Look Like
Visually, B12 injections are straightforward—vials and syringes—but the clinical decision shouldn’t be. The route, dose schedule, and monitoring should be chosen by a clinician based on your deficiency type and goals.
Benefits and Limitations to Know Before You Decide
Potential benefits
- Bypasses absorption when the gut can’t absorb B12 reliably
- Speeds replacement in cases with significant deficiency or neurologic symptoms
- Improves adherence for people who struggle with daily oral therapy
Key limitations
- Doesn’t address non-B12 causes of fatigue or neuropathy
- May not be necessary for uncomplicated low intake with reliable oral options
- Requires monitoring so clinicians can confirm response and adjust strategy
In short: injections can be the right tool, but they’re not the right answer for every scenario.
FAQ
What labs help determine how to qualify for b12 injections?
Commonly used tests include serum vitamin B12, a complete blood count (CBC), and—when results are borderline or the cause is unclear—methylmalonic acid (MMA) and/or homocysteine.
Who is most likely to need B12 injections instead of oral B12?
People with suspected or confirmed malabsorption issues (such as pernicious anemia or post-bariatric surgery) and those with significant deficiency or neurologic symptoms are often considered for injections, especially when oral therapy response is uncertain.
How will I know injections are working?
Clinicians typically track symptom improvement and repeat relevant labs. If anemia markers and/or functional markers (like MMA/homocysteine when used) improve over time, that’s a strong sign the strategy is working.
Conclusion: Decide With Cause, Not Hype
To qualify for b12 injections, focus on the fundamentals: your cause (especially absorption vs. intake), your lab evidence, and your symptom profile. In the real world, the most confident decisions come from pairing history with the right tests and using follow-up to confirm response.
Next step: Schedule a clinician visit and ask what labs you need to determine whether you meet criteria for b12 injections—including whether CBC and MMA/homocysteine are appropriate for your situation.
Discussion