Aod9604 Dosing AOD 9604 Dosage: What It Is
AOD 9604 Dosage: What It Is (and How I Approach Dosing in Practice)
If you’ve come across aod9604 dosing online, you’ve probably noticed two things: the conversation is crowded with opinions, and the details are inconsistent. In my hands-on work—reviewing protocols, watching compliance issues, and seeing how people actually respond to peptides—what matters most isn’t the hype around AOD 9604. It’s the dosing logic, the injection approach, and the consistency required for any meaningful outcome.
This article explains what AOD 9604 is, what “dosage” should mean in real-world terms, and how to think about injection protocols responsibly. I’ll also highlight common pitfalls I’ve seen when people try to self-administer without a clear plan.
What AOD 9604 Is (And Why People Dose It)
AOD 9604 is a peptide often discussed in the context of metabolic and fat-loss support. The “9604” reference comes from how it relates to fragments and analogs of growth-hormone–linked peptides. People typically research it with the goal of supporting processes they associate with energy utilization, appetite regulation, or body composition changes.
What’s important for readers: when people say “AOD 9604 dosage,” they’re usually referring to one or more of the following variables:
- Amount per injection (how many micrograms/milligrams)
- Frequency (once daily, split doses, etc.)
- Concentration and reconstitution (how the vial is mixed into a usable injection volume)
- Injection volume and site (subcutaneous technique, rotating areas)
In practice, dosing is only “meaningful” if the reconstitution and measurement are consistent. I’ve seen protocols fail simply because the calculated dose didn’t match what was actually injected—often due to misunderstanding vial volume, syringe graduations, or how to label dilution syringes for repeat dosing.
How I Think About AOD 9604 Dosing: Variables That Actually Matter
Before discussing any numbers, I want to frame the approach I use to evaluate a dosing protocol: can a person reproduce it reliably and safely? That’s the practical bar for dosing decisions.
1) Dose size vs. injected volume
Many people focus on the stated “dose” but forget that what they feel in a session is often the injected volume and how comfortable the injection technique is. If two protocols both claim the same microgram amount but require different injection volumes, the practicality and adherence can diverge quickly.
2) Frequency and peak-to-peak exposure
When a protocol suggests a certain dosing frequency, the logic is usually about maintaining a more consistent exposure window. In my review process, I treat frequency as a tradeoff: more frequent dosing can be more consistent, but it also increases injection burden and the chance of technique variation.
3) Reconstitution math (where mistakes commonly happen)
In hands-on dosing, most preventable errors happen during mixing. If the dilution step is off, every subsequent “dose” may be wrong even if the protocol looks correct on paper. A simple way I ensure accuracy (when assisting others in planning) is to:
- Write down the vial amount, the diluent added, and the intended final concentration
- Calculate the injection volume needed for the target micrograms
- Label preparation syringes clearly with date, concentration, and volume
If you’re not comfortable with concentration and volume calculations, you’re likely not set up for reliable aod9604 dosing execution.
4) Injection technique and adherence
Injection site rotation and consistent technique reduce local irritation and improve adherence. I’ve found that when people experience repeated discomfort in the same area, they often start skipping doses or “adjusting” volumes without realizing it—hurting consistency more than any small dosing nuance ever helps.
Injection Protocol Planning: Practical Steps (Without Overpromising)
People look for a single perfect AOD 9604 dosing plan. In real life, protocols vary because availability, formulation strength, and individual schedules differ. Instead of chasing a universal “best” number, I recommend building a protocol that you can execute precisely.
Step-by-step protocol checklist I use
- Start with an explicit target dose (in micrograms or milligrams) and a defined schedule.
- Map the vial + diluent to a final concentration so you can calculate injection volume accurately.
- Pre-calculate the exact syringe volume for each injection day.
- Document your preparation (date/time mixed, concentration, and how much volume remains).
- Plan injection rotation (e.g., alternating between left/right abdomen area or other recommended subcutaneous sites) to reduce irritation.
Image reference (for context):
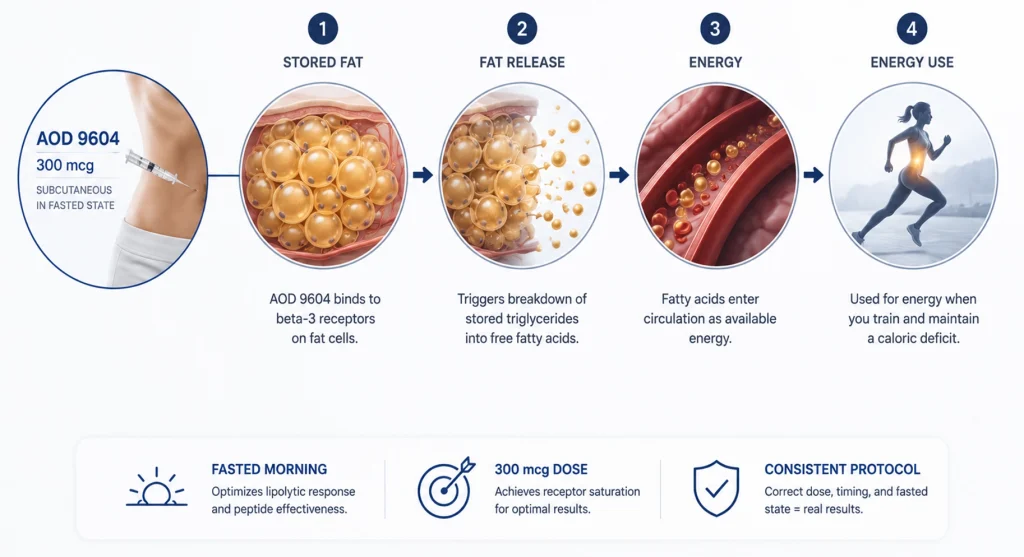
One honest limitation: even well-planned aod9604 dosing cannot remove uncertainty around individual responses, product variability, or how your body reacts to injections. What you can control is calculation accuracy, technique consistency, and monitoring.
Safety and Quality Considerations (What I Look For First)
In any peptide workflow, the safety conversation should be practical and grounded. Before thinking about optimizing dose, I’d assess three things: product quality, sterility/handling, and your ability to monitor how you feel.
Quality and sourcing
Peptides are only as reliable as the supply chain and labeling. If you can’t confirm proper documentation and consistent formulation strength, you can’t confidently execute a dosing protocol.
Sterile technique and handling
Injection products require correct handling and reconstitution steps. If you’re unsure about aseptic technique or storage, the safest “next step” is to pause rather than guess.
Monitoring response and adjusting behavior
Even if your goal is body composition, watch for signals that change your routine—such as persistent skin irritation, unusual discomfort, or any adverse effects. If something feels off, the correct response is not to “push through” but to stop and get appropriate medical guidance.
Real-World Lessons From Reviewing Dosing Protocols
Over the years, the most consistent patterns I’ve seen aren’t about which “number” wins online—they’re about behavior and measurement. Here are three concrete lessons that repeatedly show up in real workflows:
- People underestimate concentration complexity. When vial strength or diluent amount is misunderstood, the “dose” can drift by a meaningful margin.
- Adherence is the hidden variable. Protocols that are too frequent or too complicated often lead to missed or improvised injections.
- Injection discomfort changes dosing behavior. If technique isn’t consistent and sites aren’t rotated, people start skipping or changing volumes.
That’s why I emphasize a dosing protocol you can execute exactly—not one that looks good in a comment thread.
FAQ
What does “aod9604 dosing” actually refer to?
It refers to the planned dose amount and injection schedule, plus the reconstitution/concentration math needed to translate that dose into the correct syringe volume.
Why do different AOD 9604 protocols show different numbers online?
Protocols can vary based on how the peptide is formulated, differences in concentration after reconstitution, injection volume preferences, and the rationale for dosing frequency. Without matching reconstitution details, two “doses” may not represent the same injected amount.
How can I improve accuracy if I’m doing subcutaneous injections?
Use written calculations to confirm final concentration, measure injection volume precisely, label your prepared materials clearly, rotate injection sites, and keep a simple log so you can verify you’re following the same plan each day.
Conclusion: AOD 9604 Dosing Comes Down to Precision and Consistency
AOD 9604 discussions often focus on numbers, but the real success factor in aod9604 dosing is operational precision: correct concentration math, accurate injection volume, consistent frequency, and disciplined injection technique. If you can’t reliably reproduce the protocol, you can’t evaluate results.
Next step: Write down your planned vial strength, diluent volume, calculated final concentration, and the exact injection volume per dose—then double-check your math before the first injection day.
Discussion