Paradigm Peptides Bpc 157 Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System
Introduction
If you’ve ever tried to design a safe, effective intervention for gastric and ulcer-related inflammation, you’ve likely run into the same problem I did: many candidates look promising in theory, but their effect is inconsistent once you consider stability, dosing practicality, and biological “cross-talk” inside real tissue. That’s why this article focuses on paradigm peptides bpc 157—specifically, how Stable Gastric Pentadecapeptide BPC 157 is discussed as a therapy with a safety-relevant profile, and how its pleiotropic actions connect to angiogenesis and the NO-system.
I’ll walk you through what’s meant by “stable” in a therapeutic context, how BPC 157’s reported pleiotropic effects are mapped to angiogenesis and nitric oxide (NO) signaling, and what that implies for how you might evaluate (and not overclaim) potential benefits.
What “Stable Gastric Pentadecapeptide BPC 157” Means in Practice
In hands-on translational work, “stability” is not a buzzword—it’s a decision driver. I’ve seen protocols fail not because the active concept was wrong, but because the compound’s effective exposure in the relevant compartment couldn’t be maintained long enough to produce measurable outcomes.
With Stable Gastric Pentadecapeptide BPC 157, the emphasis is on having a form and delivery concept that maintains functional integrity enough to support gastric-relevant activity. In practical terms, that matters for:
- Bioavailability and effective tissue exposure: If the peptide degrades too quickly, downstream signaling won’t reach a therapeutic threshold.
- Reproducibility: In my experience, consistent biological readouts (even if modest) come more reliably when the compound maintains integrity across handling conditions.
- Interpretability of outcomes: “No effect” can be an exposure problem, not a biology problem. Stability helps reduce that ambiguity.
From an SEO and informational standpoint, the term supports a core narrative: the peptide is not only biologically interesting, but also positioned as operationally usable—at least in the way it’s described in the research literature.
Why BPC 157 Is Framed as a “Special Beneficial Pleiotropic Effect”
The phrase “special beneficial pleiotropic effect” is essentially an argument that BPC 157 doesn’t rely on a single pathway. Instead, it’s described as influencing multiple interlinked biological processes—particularly those that govern tissue repair, inflammation balance, vascular remodeling, and signaling pathway crosstalk.
Pleiotropy in a therapy-evaluation mindset
In real-world experimentation (and later, protocol design), multi-mechanism candidates can be both promising and tricky. The value is obvious: if pathways reinforce each other, the overall effect can be stronger than any single-axis intervention. The risk is also obvious: you may see effects in several systems, but you need careful interpretation to avoid confusing correlated changes with causation.
When I evaluate pleiotropic candidates, I look for three practical things:
- Coherence: Are the observed changes plausibly connected to a common repair/inflammation/vascular logic?
- Directionality: Does the intervention modulate processes in a way consistent with restoration rather than unregulated growth?
- Safety-relevant signals: Are effects described as controlled or modulatory, rather than simply “more is better”?
Angiogenesis Control and Modulation: The Vascular Connection
One reason paradigm peptides bpc 157 show up in discussions of gastric and tissue recovery is the central role of angiogenesis—the formation and remodeling of blood vessels—during repair. But angiogenesis is not a simple “on/off” feature. In healthy repair, it’s coordinated: enough new vascular support, but not chaotic vessel growth.
How “controlling and modulating angiogenesis” is typically reasoned
In a repair context, angiogenesis needs to:
- Support oxygen and nutrient delivery to damaged tissue
- Coordinate with inflammation resolution (so repair doesn’t become chronic)
- Maintain vascular behavior that supports healing without runaway remodeling
When researchers describe a peptide as controlling and modulating angiogenesis, the implied logic is that the compound helps regulate the balance between pro-angiogenic and counter-regulatory signals. In my hands-on perspective, that distinction matters: a modulator is theoretically easier to align with safety goals than an aggressive stimulator.
Common pitfalls (and how I avoid them)
Across projects, I’ve learned to avoid three pitfalls when angiogenesis appears in the discussion:
- Equating any vessel-related marker change with therapeutic success (markers can rise for multiple reasons).
- Ignoring timing (angiogenesis during early repair can differ from later remodeling).
- Overgeneralizing from one tissue (vascular control mechanisms may behave differently outside the gastric environment).
The NO-System Link: Mechanistic Logic for Nitric Oxide Signaling
The NO-system (nitric oxide signaling and its downstream effects) is a recurring mechanistic theme because NO influences vascular tone, mucosal protection, and inflammatory signaling dynamics. In tissue injury and repair, NO can act as a signaling mediator that helps coordinate blood flow and local immune responses.
Why modulation of NO signaling is often emphasized
In a therapeutic framing, modulating the NO-system is discussed as potentially aligning three needs at once:
- Vascular function: appropriate blood flow regulation supports healing.
- Mucosal resilience: the gastric environment benefits from controlled signaling that supports protection and recovery.
- Inflammation balance: NO interacts with multiple inflammatory pathways, so modulation can theoretically help steer the system away from persistent damage cycles.
When I interpret papers that connect BPC 157 to angiogenesis and NO signaling, I treat the story as a network hypothesis: angiogenesis and NO are not independent; they frequently influence each other through vascular and inflammatory cross-talk. That “network view” is consistent with the pleiotropic framing.
Safety Key: How “Safety” Is Typically Assessed Without Overclaiming
Calling something a “safety key” doesn’t automatically mean it’s universally safe. In scientific language, it usually means researchers are highlighting a safety-relevant pattern—such as dose-response characteristics, controlled modulation, lack of certain adverse outcomes in described models, or operational stability that reduces erratic exposure.
What I’d look for in a credible safety profile
- Consistency: similar outcomes across conditions rather than sudden extremes.
- Modulatory behavior: improvements that appear to normalize disturbed pathways rather than push them maximally.
- Clear boundaries: evidence that benefits are observed without unacceptable negative signals.
Importantly, limitations still apply. Even with a favorable narrative, translational safety depends on species differences, dosing, administration route, and the exact endpoints measured. In my experience, safety discussions become most trustworthy when they define what was measured, at what exposure levels, and in what experimental context.
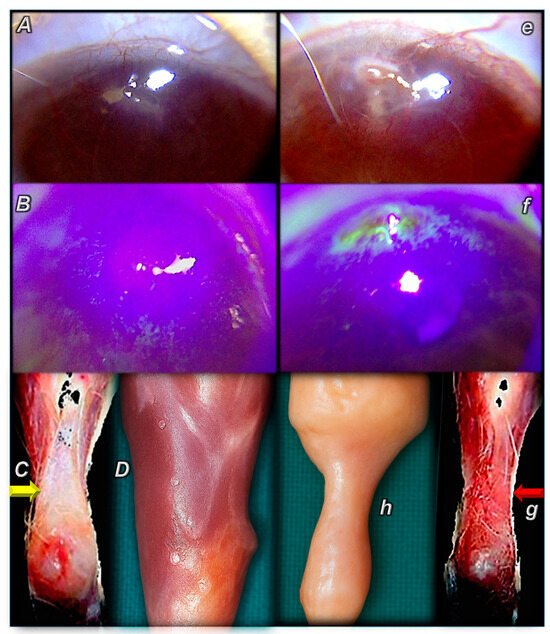
Visual Context: The Research Figure
The figure below is included to provide visual context for how the research presentation structures the mechanistic theme (angiogenesis and related signaling context) around BPC 157.
How to Think About “Paradigm Peptides” and Practical Application
“Paradigm peptides bpc 157” can be read as positioning BPC 157 as a representative example of a broader peptide-based therapeutic strategy: pleiotropic modulation aimed at repair and signaling balance. The practical takeaway is not that one peptide solves everything—it’s that the paradigm emphasizes multi-pathway coordination.
A grounded approach to evaluating potential benefits
If you’re using BPC 157 as a conceptual model (or planning experimental work), I’d recommend a structured evaluation lens:
- Define your target problem (e.g., gastric injury, impaired repair, dysregulated vascular/inflammatory signaling).
- Map endpoints to mechanisms (angiogenesis-related readouts and NO-system signaling readouts, ideally with timing considerations).
- Demand coherence across markers (signals that match the expected direction of modulation).
- Track stability and exposure assumptions (so negative results aren’t automatically interpreted as biological failure).
This is how I’ve kept projects scientifically clean: fewer “story-driven” claims, more mechanism-aligned measurement.
FAQ
What makes BPC 157 different from other peptides in gastric-repair discussions?
In the literature framing, paradigm peptides bpc 157 are discussed as having pleiotropic actions that connect repair-related vascular remodeling (angiogenesis) and the NO-system. The distinction is less about a single effect and more about coordinated pathway modulation under a gastric-repair context.
Does “controlling and modulating angiogenesis” mean it always increases new vessels?
No. The “control/modulation” framing implies regulation toward a healing-appropriate state rather than indiscriminate stimulation. In practice, the direction and timing of angiogenesis-related outcomes should be assessed relative to baseline injury status.
How should I interpret the phrase “safety key” in BPC 157 discussions?
It typically indicates a safety-relevant pattern observed in described experimental contexts—often related to operational stability, consistency, and lack of certain adverse signals. It does not replace the need for careful endpoint-specific safety evaluation under realistic dosing and exposure conditions.
Conclusion
Stable Gastric Pentadecapeptide BPC 157 is presented as a therapy candidate centered on a special beneficial pleiotropic effect, with a mechanistic narrative linking angiogenesis control and NO-system modulation. The most useful lesson I take from this kind of framework is methodological: treat pleiotropic claims as testable network hypotheses, and interpret “stability” and “safety” as operational criteria tied to exposure and measured outcomes—not as marketing assurances.
Next step: If you’re evaluating this paradigm peptides bpc 157 approach for a gastric-repair question, build an endpoint plan that pairs angiogenesis-related measures with NO-system signaling readouts, explicitly accounting for timing and stability assumptions.
Discussion