B12 Injection Or Supplement Are Vitamin B12 Shots Right for You?
If you’re considering a b12 injection or supplement, you’re probably dealing with one of the same frustrating realities I’ve seen in clinic: symptoms that feel “non-specific” (fatigue, brain fog, tingling) but still demand a careful, evidence-based decision. In this guide, I’ll break down when B12 shots make sense, when supplements are the better first step, and how to choose an approach that matches your cause—not just your lab number.
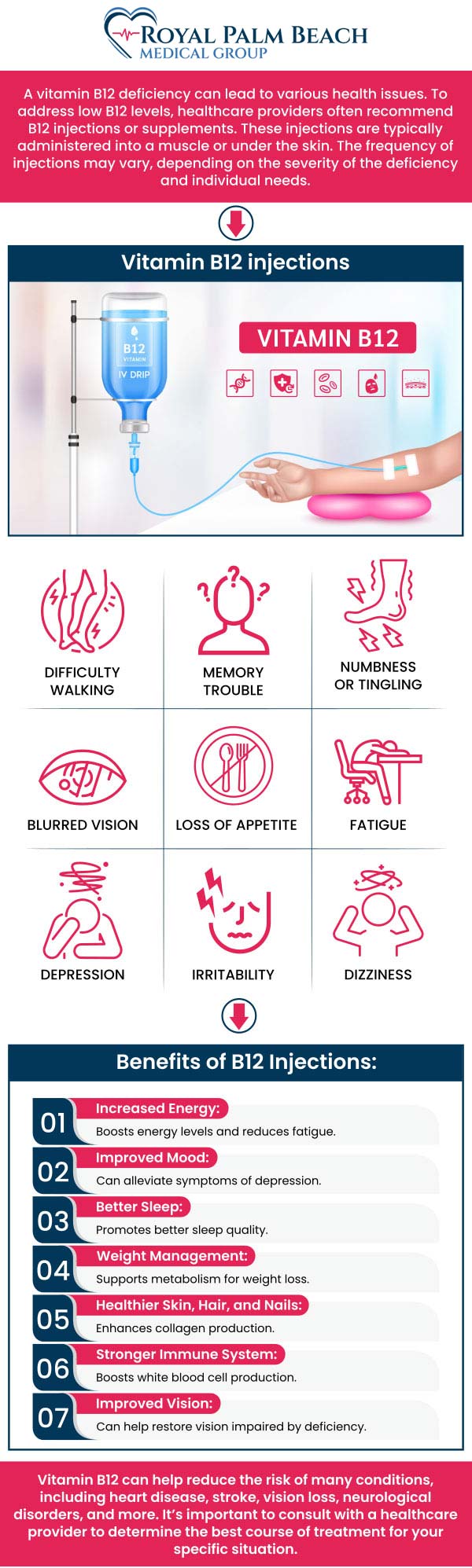
Quick context: what a B12 injection actually does
Vitamin B12 (cobalamin) is required for red blood cell production and normal nerve function. When people say “B12 shots,” they usually mean an intramuscular injection designed to deliver B12 directly into circulation, bypassing absorption steps that can fail in some medical conditions.
In my hands-on work, the key insight is this: the “right” method depends less on whether B12 is present and more on why B12 is low (or not being used effectively). If absorption is the bottleneck, a shot can be a practical way to get to therapeutic levels without relying on the gut.
Are B12 shots right for you? Use-case decision framework
Here’s how I typically sort candidates. Think of it as matching symptoms and likely cause to the route of replacement.
Injections tend to fit better when absorption is likely impaired
- Known pernicious anemia (autoimmune causes of poor intrinsic factor production).
- History of gastric/intestinal surgery (for example, certain bariatric procedures).
- Inflammatory or malabsorption conditions that reduce nutrient uptake.
- Medication-related absorption issues (some long-term acid suppression or other therapies can contribute to low B12 in susceptible people).
- Significant deficiency with neurologic symptoms where clinicians prioritize prompt repletion.
In one real-world pattern I’ve observed over multiple visits, people with clear malabsorption risks often try oral b12 replacement first, then still land in the “why isn’t it improving?” loop. When we switch to a b12 injection or supplement route that doesn’t depend on intestinal absorption, lab markers and symptom trends can improve more predictably.
Supplements (often oral) may be a better first step when absorption is likely intact
- Mild to moderate low B12 identified on routine bloodwork without strong risk factors for malabsorption.
- You prefer a non-procedural option and can reliably take doses as directed.
- No neurologic symptoms or severe deficiency picture.
Oral B12 can still work even when absorption varies, because at sufficiently high doses, a small percentage can absorb passively. The logic is straightforward: if your body can take up at least some B12—even imperfectly—oral replacement may be enough.
When your symptoms don’t match B12 deficiency, neither shots nor supplements are the answer
Fatigue, numbness, or cognitive changes can come from many causes (iron deficiency, folate issues, thyroid problems, diabetes-related neuropathy, sleep disorders, medication side effects). If you’re treating symptoms without confirming deficiency and cause, you can end up spending time and money while the real driver continues.
What I look at before recommending a b12 injection or supplement plan
I avoid “one-size-fits-all” prescribing in my approach, and I encourage readers to do the same. A thoughtful plan usually includes both labs and clinical context.
1) Lab values that inform the likely cause
Common starting points include:
- Serum B12 (baseline level, though it can be imperfect).
- Methylmalonic acid (MMA) and/or homocysteine (can help confirm functional deficiency).
- Complete blood count (CBC) (helps evaluate anemia patterns).
2) Symptom severity and timing
Neurologic symptoms are the critical branch. If tingling, numbness, balance issues, or other nerve-related changes are present, clinicians often consider a more urgent repletion strategy. That urgency is one reason B12 injections may be prioritized in certain cases.
3) Practical constraints that affect adherence
In my experience, the “best” plan is also the one you can stick with. If someone dislikes injections or can’t attend appointments, an oral b12 injection or supplement approach that they can take consistently may work better than a medically ideal plan they won’t follow.
Benefits and limitations: shots vs supplements
Below is a practical comparison I use to set expectations without hype.
| Factor | B12 injection | Oral supplement (b12 injection or supplement approach) |
|---|---|---|
| Absorption dependency | Largely bypasses gut absorption | Relies on gastrointestinal absorption (with some passive uptake at higher doses) |
| Onset of repletion | Often faster, especially in marked deficiency or malabsorption scenarios | Can be effective but may take longer depending on cause and dose |
| Convenience | Requires injections and scheduling | No clinic visits needed; easier to incorporate into routine |
| Side effects profile | Injection site discomfort possible; clinician administration reduces technique issues | GI upset is possible in some people; generally avoids injection-related risks |
| Best-fit situations | Malabsorption, pernicious anemia, certain neurologic symptom patterns | Milder deficiency or when absorption is likely intact and adherence is strong |
| Costs | May involve professional administration and supplies | Often lower cost; depends on formulation and dose |
How to talk to your clinician (and avoid common pitfalls)
If you’re deciding between a b12 injection or supplement, I recommend bringing a short, structured summary. In my clinic, it speeds up decision-making and reduces guesswork.
- Your symptoms (include onset date and whether any neurologic symptoms exist).
- Your lab results (B12, CBC, and any MMA/homocysteine if available).
- Risk factors (gastric surgery, pernicious anemia history, malabsorption conditions, relevant medications).
- Your preferences and constraints (injection comfort, appointment availability, ability to take daily/weekly supplements).
Common pitfall: relying on “B12 is low” alone without verifying functional deficiency (MMA/homocysteine) when symptoms are significant or the cause is unclear. Another pitfall I’ve seen is stopping treatment too early without rechecking labs or trending symptoms.
Sample decision scenarios from real-world patterns
Scenario A: Mild deficiency, no malabsorption risk
I’d typically lean toward an oral b12 replacement strategy first, paired with a follow-up lab plan. The goal is to see a measurable trend without jumping to injections immediately.
Scenario B: Confirmed pernicious anemia or clear malabsorption
In this scenario, a b12 injection strategy often makes more sense because the body’s ability to absorb B12 is impaired by the underlying mechanism. The decision is less about preference and more about physiology.
Scenario C: Neurologic symptoms with low B12 markers
Here, the approach needs speed and medical supervision. If neurologic symptoms are present, I generally recommend prioritizing clinician-guided repletion and monitoring rather than trying to “experiment” with delayed supplementation alone.
FAQ
Do b12 injection or supplement plans work if my B12 level is only slightly low?
Often yes, but it depends on symptoms and whether functional deficiency is present. If you have concerning symptoms, clinicians may check MMA and homocysteine to confirm that B12 deficiency is truly affecting metabolism—not just reflecting a borderline number.
Will B12 shots be better if I can’t tolerate pills?
They can be a practical alternative when adherence is likely to fail with oral supplements due to intolerance, scheduling barriers, or GI side effects. The best plan still depends on cause—especially if malabsorption is suspected.
How long should it take to see improvement?
Trends vary by cause and symptom type. Blood markers may shift sooner than neurologic symptoms. In my experience, a clinician-guided follow-up schedule with repeat labs and symptom tracking is the most reliable way to judge whether the plan is working.
Conclusion: choose the route that matches the cause
Whether you choose a b12 injection or supplement, the most important decision is not the brand—it’s the reason your B12 status is low and how your body handles absorption. Shots often fit when malabsorption or neurologic concerns are present. Supplements can be a smart first step when absorption is likely intact and you can take them consistently.
Next step: Gather your latest B12 and CBC results (and any MMA/homocysteine if you have them), list your symptoms with dates, and schedule a clinician visit to decide whether your situation calls for an injection strategy or an oral b12 replacement plan with a clear follow-up timeline.
Discussion