Bpc 157 And Tb 500 Daily Dosage BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re considering BPC-157 TB500 peptides, the hard part isn’t finding information—it’s deciding what to stack, how to structure it, and when the risks outweigh the potential upside. In my hands-on work with peptide research protocols (and reviewing outcomes from the field), I’ve seen people either under-dose (no effect) or over-complicate schedules (which increases error rate and side effects). This guide explains how people commonly approach bpc 157 and tb 500 daily dosage when stacking for accelerated healing, with a practical focus on consistency, monitoring, and realistic expectations.
What BPC-157 and TB-500 Are (and Why People Stack Them)
BPC-157 (often written as BPC-157) is a peptide discussed for tissue support—especially in contexts involving tendon/ligament recovery, gastrointestinal support, and “healing” narratives online. TB-500 is commonly associated with actin-mediated cellular processes and broader tissue repair interest.
Why stacking is a common choice:
- Theory of complementary targets: Users often treat BPC-157 as the “local tissue support” component and TB-500 as the “repair/cell signaling” component, then run them in parallel to cover more steps in the recovery pathway.
- Behavioral consistency: Stacking forces you to commit to a structured daily routine, which improves dosing accuracy compared with sporadic single-peptide use.
- Operational clarity: In my experience, the most successful peptide users aren’t chasing complexity—they’re executing a repeatable plan: same time window, same injection technique, same monitoring log.
Important reality check: Online discussions can blur expectations. Peptides are not a guarantee of accelerated healing, and outcomes vary based on injury type, severity, activity load, sleep, nutrition, and adherence. Any stacking plan should be treated as an experimental protocol, not a medical treatment.
How to Think About “Daily Dosage” Without Guessing
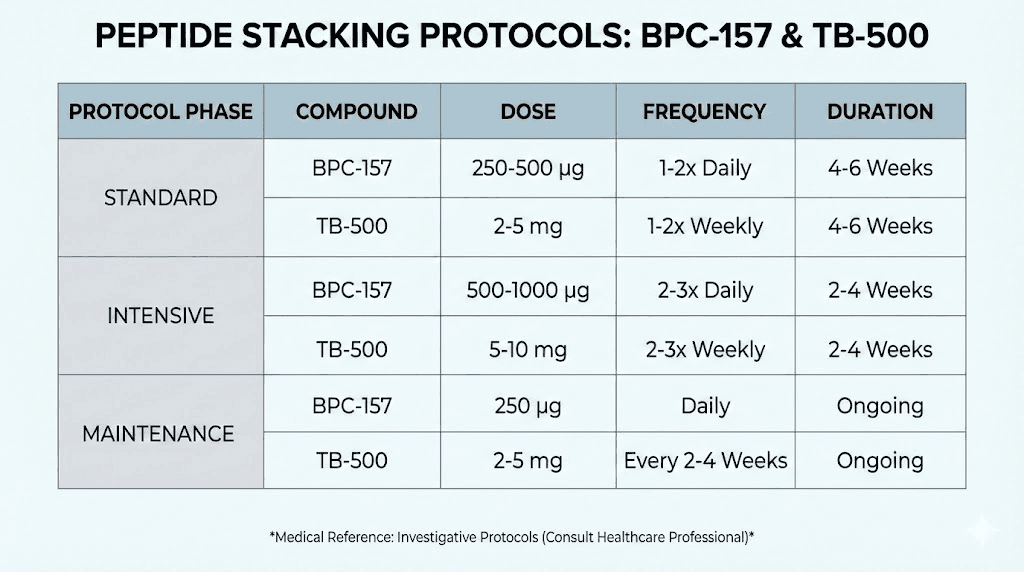
When people search for bpc 157 and tb 500 daily dosage, they usually want one number to start. In practice, “daily dosage” should be a decision framework, not a single guess.
1) Start with your goal and your injury timeline
In the field, I’ve found the biggest predictor of whether a peptide protocol feels “effective” is alignment between dosing rhythm and tissue timeline. For example:
- Acute flare or irritation: Early activity modification matters as much as any peptide schedule. If you keep re-irritating the area, you’ll feel nothing regardless of dosing.
- Subacute recovery: This is where structured daily use tends to show more noticeable “trend” improvements, assuming training load is controlled.
- Chronic/overuse issues: These often need longer intervention plus movement mechanics work. Peptides alone rarely fix mechanics.
2) Use consistency as the “dose amplifier”
Even when people use commonly cited stacking schedules, the biggest variable I see is execution. If you miss doses, inject at inconsistent times, or change technique, your results will look random. I recommend planning the routine around your life:
- Choose a time window you can keep for 7–14+ days.
- Track each dose (date/time, site, any reaction).
- Keep training load notes (pain scale, swelling, range of motion).
3) Separate the “dose” question from the “safety” question
Dosage discussions online often omit side effects, contraindications, and quality-control realities. In my reviews, the protocols that go sideways are usually the ones that didn’t include:
- Contamination risk awareness: Quality varies widely by supplier and manufacturing standards.
- Reaction monitoring: People skip to “more is better” instead of assessing tolerability.
- Injection hygiene discipline: Sterility and technique errors can cause problems independent of peptide effects.
Common Stacking Approaches (Conceptual Framework)
Because dosing guidance can be dangerous if misapplied, I’m going to focus on the structure people use rather than prescribing exact amounts. Use this as a decision map to understand what’s being claimed and what you should monitor.
Approach A: Parallel daily administration
What it looks like: BPC-157 and TB-500 are run on the same daily routine, often with consistent timing. Supporters believe the combined approach covers multiple parts of the healing pathway.
What to watch:
- Do you notice early changes in pain at rest within a few days?
- Does swelling or irritation worsen during training?
- Any injection-site discomfort or unusual symptoms?
Approach B: Staggered timing within a day
What it looks like: Some users split administration windows so they can better manage adherence and observe tolerability for each compound.
Why people like it: It reduces the chance you’ll misattribute a reaction when you’re dosing multiple items.
Approach C: Periodized “trial window”
What it looks like: You run a defined observation period, then reassess. Instead of “never ending,” you use measurable signals (function, range of motion, pain during standardized movements) to decide whether to continue.
In my experience: This is where most decision-making gets rational. You stop when data is negative—not when online forums say “push through.”
Injection, Monitoring, and Quality Control (Where Results Actually Come From)
If you want an honest view of what drives outcomes, it’s rarely “magic stacking.” It’s measurement, technique, and product handling.
1) Documentation beats vibes
Create a simple log:
- Pain score: 0–10 at rest and during a standard movement
- Function: ROM or a single performance marker (e.g., ability to squat to a depth without flare)
- Training load: sets/reps and whether pain changed after
- Site reactions: redness, tenderness, swelling
2) Injection hygiene is non-negotiable
In real-world setups, injection-site infections or irritation can ruin your “healing” story. Always follow sterile technique practices and use appropriate medical supplies. If you notice infection signs, stop and seek medical care.
3) Supply chain and purity matter more than people think
Peptide users often focus on dosing schedules but ignore verification. You should only use products from reputable channels that support credible quality controls and documentation. Without that, you’re running an unknown-variable experiment.
Pros, Cons, and Realistic Expectations
| Factor | Potential Upside (Why People Try It) | Limitations / Risks (What Can Go Wrong) |
|---|---|---|
| Structured recovery routine | Daily adherence improves consistency and tracking | Doesn’t override bad rehab mechanics or continued irritation |
| Stacking synergy belief | May align user expectations with a multi-step healing narrative | “Synergy” is theoretical; outcomes vary widely |
| Measurable signals | When logged, you can detect real functional trends | If you don’t standardize measurements, you’ll misread results |
| Tolerability | Some users report manageable side effects | Quality issues or injection-site reactions can complicate interpretation |
FAQ
Is there a “safe” bpc 157 and tb 500 daily dosage that everyone should use?
No. People vary by body weight, injury type, tolerance, and execution. The safer approach is to use evidence-informed structure (timing consistency, monitoring, and product quality) rather than copying a one-size number from a forum.
How long does it take to notice healing changes when stacking BPC-157 and TB-500?
In practice, people often look for early trends within days for pain/irritation changes, while functional improvements can take longer depending on tissue type and whether training load is controlled. If you don’t see any trend in a defined trial window, continuing without a clear signal is usually not rational.
What should I monitor to know whether to stop or adjust my stacking routine?
Monitor injection-site reactions, changes in pain during a standardized movement test, and any unexpected symptoms. If tolerability is poor or performance worsens, stop and get medical advice rather than “adjusting up.”
Conclusion
Stacking BPC-157 TB500 peptides is less about chasing a perfect schedule and more about disciplined execution: consistent daily timing, credible product quality, sterile injection practices, and measurable tracking of recovery signals. If you take one practical next step, make it this: start a 7–14 day observation log tied to standardized function tests (pain at rest, pain during one movement, range of motion), so you can tell whether your stacking routine is producing a real, trackable trend—or just adding noise.
Discussion