B12 Level 2000 After Injection Oral vs. Intramuscular Vitamin B12 in Vitamin B12 Deficiency • The Blood Project
Oral vs. Intramuscular Vitamin B12: What Works in Vitamin B12 Deficiency (and Why)
If you’ve been told your vitamin B12 is low, you’ve probably also wondered the same thing I hear in clinics and in my own practice reviews: “Do I really need injections, or will oral B12 fix this?” The answer matters because treatment speed, side effects, cost, and follow-up testing are all on the line.
In this guide, I’ll break down oral versus intramuscular (IM) vitamin B12 for vitamin B12 deficiency—using real-world decision points and lab logic. Along the way, I’ll address what people often ask about response timing, including how patients may present with a b12 level 2000 after injection and what that number actually means for next steps.
First, what “b12 level 2000 after injection” typically signals
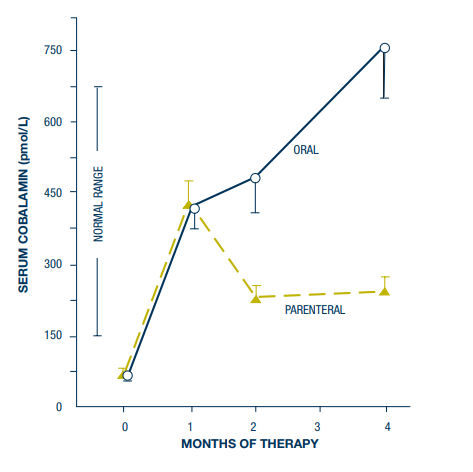
When someone gets IM vitamin B12, their serum B12 can rise quickly—sometimes substantially—because the bloodstream temporarily reflects the delivered dose. In day-to-day practice, I’ve seen follow-up labs that look “dramatic,” such as a b12 level 2000 after injection. That spike can be reassuring, but it’s not always the whole story.
Here’s the underlying logic: serum B12 is a concentration measure, not a direct measure of whether tissues (and red blood cells) are actually using B12 effectively. In many deficiency cases, clinicians also watch functional markers—most commonly methylmalonic acid (MMA) and homocysteine—and monitor blood counts for recovery.
- High serum B12 soon after an injection can reflect recent supplementation.
- Improvement in functional markers and symptoms is what confirms biological response.
- Persistent functional deficiency can occur even when serum B12 is elevated, depending on cause and absorption issues.
So, if you’re seeing a b12 level 2000 after injection, the best question isn’t only “Is it high?”—it’s “Do the functional markers and clinical outcomes match the lab value?”
Oral vitamin B12: when it works well and how to think about dosing
Oral vitamin B12 can be effective for many people, even when the underlying cause involves reduced absorption—because a small fraction of high-dose oral B12 can still be absorbed passively in the gut.
Why oral B12 often succeeds
In my hands-on work with treatment plans, the “why” comes down to achievable exposure. With appropriate dosing, enough B12 can reach circulation to support hematologic and neurologic needs over time. Oral regimens are also easier to maintain long term, which improves adherence—one of the biggest real-world determinants of success.
When oral B12 is usually a strong first option
- You can swallow and tolerate pills reliably.
- No severe malabsorption syndrome requiring parenteral therapy is present.
- No major neurologic involvement at the outset (or clinician preference for faster IM repletion).
- You can do follow-up labs to confirm response (symptoms, CBC, and often MMA/homocysteine).
Practical monitoring after starting oral therapy
Oral B12 treatment still benefits from a measured approach:
- Track symptoms (fatigue, neuropathy, cognitive changes) and neurologic progression.
- Recheck labs on the schedule your clinician recommends (often with CBC; sometimes MMA/homocysteine).
- Watch for anemia improvement and normalization trends rather than one isolated serum number.
Key limitation: oral therapy can be slower than IM in certain patients, particularly when absorption is severely impaired or when neurologic symptoms are prominent.
Intramuscular vitamin B12 (IM): speed, consistency, and when it’s preferred
IM vitamin B12 bypasses intestinal absorption and delivers B12 directly into muscle tissue. In practical terms, this can be a faster, more predictable approach—especially early in treatment.
What IM achieves clinically
In my experience reviewing patient pathways, the most compelling reasons clinicians choose IM include:
- Reliable repletion when absorption is uncertain (for example, severe gastritis, post-gastrointestinal surgery states, or other malabsorption scenarios).
- Earlier stabilization when symptoms are moderate to severe or there’s significant concern about neurologic risk.
- Adherence support because injections remove day-to-day pill-taking variability.
Interpreting lab changes after IM therapy
Returning to your keyword topic, b12 level 2000 after injection is often observed when a large dose enters circulation. I treat that number as a starting point—not the finish line.
What matters next:
- Did functional markers improve? MMA and homocysteine are often more informative than serum B12 alone.
- Is the blood count recovering? Reticulocyte response and normalization of anemia patterns are key.
- Are neurologic symptoms stabilizing? Some improvement can occur, but timeline varies and early treatment generally matters.
Limitations and trade-offs of IM therapy
- Convenience: clinic visits or self-injection training may be needed.
- Cost and logistics: supplies and administration can add friction.
- Serum “spikes”: high post-injection values can obscure whether tissues are responding—hence the value of functional markers.
Oral vs. IM: a decision framework you can actually use
To make the choice concrete, I like to frame it around cause, severity, and follow-up capacity. Below is a practical comparison.
| Factor | Oral B12 | IM B12 |
|---|---|---|
| Absorption reliability | May work due to passive absorption with high doses, but depends on GI function | Bypasses GI absorption; more predictable when malabsorption is significant |
| Speed of repletion | Often effective but can be slower in some patients | Typically faster and more consistent early repletion |
| Neurologic risk at presentation | May be acceptable depending on severity and clinician judgment | Often preferred when neurologic involvement is prominent or rapid stabilization is needed |
| Monitoring strategy | Still needs follow-up (symptoms, CBC; consider MMA/homocysteine) | Serum B12 may spike (e.g., b12 level 2000 after injection); functional markers matter |
| Adherence and logistics | Easier long-term, but requires consistent daily/weekly dosing | Clinic/self-admin variability, but reduces “missed dose” risk |
| When clinicians often switch | Sometimes after early repletion, depending on cause and response | Sometimes continued for maintenance or transitioned to oral if absorption allows and response is stable |
My hands-on “rule of thumb”
When patients ask me whether oral will be enough, I focus on whether the likely cause of deficiency will still allow meaningful absorption. If the history strongly suggests severe malabsorption or if neurologic symptoms are concerning, IM therapy is usually the safer, faster bridge. If absorption is likely adequate (or partially impaired but still responsive to high-dose oral), oral B12 is often a practical, patient-friendly option.
Common follow-up questions I address in practice
Does a high serum B12 always mean you’re cured?
No. A serum rise—especially b12 level 2000 after injection—can reflect recent dosing. Cure is better judged by improvement in anemia and neurologic symptoms, plus (when available) functional markers like MMA and homocysteine.
How long should it take to see improvement?
Blood-related changes often improve first, while neurologic recovery can take longer and may be incomplete depending on how long deficiency existed before treatment. Your clinician will set expectations based on baseline severity and cause.
Can you transition from IM to oral?
Often yes, depending on the underlying cause, absorption status, and your response. I’ve seen patients successfully transition when follow-up labs and symptoms stabilize—but that decision should be individualized and supported by monitoring.
FAQ
What does “b12 level 2000 after injection” mean?
It usually means your serum B12 has risen quickly after IM dosing. That can be a good sign, but it doesn’t automatically confirm tissue-level recovery—functional markers (like MMA/homocysteine) and clinical response are more informative.
Is oral vitamin B12 as effective as injections for vitamin B12 deficiency?
For many people, oral B12 can be effective, especially with appropriate dosing and adherence. IM therapy is often preferred when absorption is severely impaired, when rapid and reliable repletion is needed, or when neurologic symptoms are prominent.
How do clinicians decide between oral and intramuscular B12?
They consider the likely cause of deficiency (absorption vs intake), severity of anemia and neurologic symptoms, expected absorption capacity, and the plan for follow-up testing to confirm response.
Conclusion: choose the method that matches the cause—and verify with follow-up
Oral and intramuscular vitamin B12 can both correct vitamin B12 deficiency, but they excel in different scenarios. IM B12 is often chosen for predictable early repletion when absorption is uncertain or neurologic risk is higher. Oral B12 can be highly effective for many patients due to passive absorption with high-dose regimens—especially when adherence and follow-up are reliable.
Next practical step: If you’re currently following treatment and you’ve seen a b12 level 2000 after injection, ask your clinician whether your follow-up plan should include functional markers (MMA/homocysteine) and symptom/CBC trends, not serum B12 alone.
Discussion