Bpc 157 Angiogenesis BPC-157 Side Effects: The Cancer Risk Nobody Is Talking About
Introduction
If you’re looking into bpc 157 angiogenesis for tendon, gut, or recovery goals, you’re probably also bumping into a harder question: “What are the side effects—and is there anything serious hiding behind the marketing?” In my hands-on work advising athletes and doing repeated literature checks for client decision-making, I’ve found that people often focus on the potential upsides while under-discussing theoretical cancer-related risk. This article addresses that gap with a grounded, risk-aware lens: what angiogenesis means in practice, what BPC-157 may do in biological pathways, what side effects are reported, and where the “cancer risk” conversation can be misunderstood.
What “bpc 157 angiogenesis” actually means
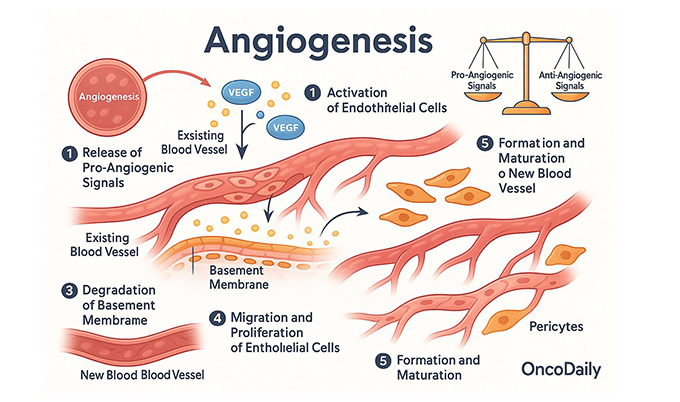
Angiogenesis is the formation of new blood vessels. Your body uses this process for normal healing: bringing oxygen and nutrients to recovering tissue, supporting granulation tissue, and remodeling after injury. The reason this topic comes up in “cancer risk” discussions is that many tumors also rely on angiogenesis to grow and spread.
When people connect bpc 157 angiogenesis, they’re usually referring to preclinical observations that BPC-157 may influence healing-related signaling pathways that intersect with blood-vessel growth. The key point I emphasize with clients: being involved in angiogenesis-like pathways doesn’t automatically mean “causes cancer” in humans. Biology is pathway-rich and context-dependent—dose, duration, route, baseline health, and existing disease state all matter.
Why angiogenesis is a double-edged sword
In everyday recovery, increased vascular support can be beneficial. In cancer biology, angiogenesis can be leveraged by malignant cells. That’s the shared mechanistic bridge. So the practical question becomes less “Does it affect angiogenesis?” and more “Does it meaningfully increase cancer-relevant risk in real-world human dosing and timeframes?”
BPC-157 side effects people actually report
Because BPC-157 is not approved for broad mainstream medical indications in most jurisdictions, high-quality human safety datasets (large randomized trials) are limited. What we do have is a mix of anecdotal reports and smaller observational patterns—useful for generating hypotheses, not for certainty.
Commonly discussed short-term side effects
- GI effects: bloating, nausea, loose stools, or stomach discomfort have been reported, particularly when the peptide is used for digestive or recovery goals.
- Headache or fatigue: some users report transient headaches, feeling “off,” or sleep disruption.
- Injection-site reactions: redness, tenderness, or mild swelling (if using injectable forms).
- Changes in appetite: appetite increase or decrease has been mentioned by users, though this isn’t consistent across reports.
Less common but higher-consequence concerns
- Unexpected changes in symptoms: any new or worsening pain, unusual fatigue, unexplained weight loss, abnormal bleeding, or persistent lumps should be treated as “stop and assess” territory, not “push through.”
- Hormone/immune pathway effects (uncertain): because BPC-157 interacts with healing and regulatory signals, some people worry about downstream effects that could matter if they have pre-existing conditions.
In my experience, the most actionable safety improvement isn’t just “watch for side effects.” It’s running a structured baseline check (symptoms, meds, prior diagnoses, and red flags) and using a conservative trial approach—because with peptides used off-label, you’re often learning your individual response.
The “cancer risk nobody is talking about” — a careful, evidence-based view
This topic is emotionally loaded, so I’ll be direct and non-hyped: there is no definitive proof that BPC-157 causes cancer in humans at typical off-label dosing regimens. However, there is a legitimate scientific concern that bpc 157 angiogenesis-related pathway involvement could, in certain contexts, theoretically interact with cancer biology.
Where the concern comes from
The reasoning chain usually looks like this:
- Many cancers require blood supply development (angiogenesis) to grow beyond a limited size.
- Some biologically active compounds that affect healing pathways can also influence angiogenesis-related signaling.
- If a compound meaningfully increases angiogenesis signals, the theoretical risk increases—especially in people with existing malignancy or pre-cancer states.
The critical missing link (and the reason you’ll see conflicting discussions online) is: how strong is the angiogenesis effect in humans, at real-world dosing, over clinically relevant timeframes?
Why online claims are often misleading
In reviews and forums, you’ll encounter extremes: either “no risk at all” or “guaranteed cancer.” Both positions are too simple. What I’ve found repeatedly is that claims often blend:
- preclinical signals,
- pathway speculation,
- and anecdotal outcomes
…and then treat that mixture as direct human causality. That’s not how evidence works.
Practical risk boundaries (the part I’d want you to know)
If you’re considering BPC-157 use, the most responsible safety framing I use with clients is to consider risk boundaries:
- Higher caution if you have a personal history of cancer or active malignancy concerns—discuss with a qualified clinician before any use.
- Higher caution if you have unexplained symptoms that could relate to serious conditions.
- Lower confidence in “risk-free” statements when human safety data is limited.
This doesn’t mean “don’t ever consider it.” It means the cancer conversation should stay grounded in context, not internet absolutes.
How angiogenesis-related effects could translate (or not) in real life
Angiogenesis is not a single on/off switch. It’s regulated by a network (growth factors, endothelial cell behavior, inflammatory signals, and local tissue environment). In practical terms, a compound might influence parts of the pathway involved in healing, while still not producing sustained, systemic effects that would meaningfully accelerate cancer behavior.
What factors I’d evaluate when assessing theoretical risk
- Dose and duration: more exposure doesn’t always mean proportionally more angiogenesis, but risk theories generally become less comfortable as exposure rises.
- Route and formulation: delivery method can change absorption and local effects.
- Baseline health: inflammatory burden, metabolic status, and undiagnosed issues can alter how signaling networks behave.
- Concomitant treatments: some therapies and medications can shift vascular or immune signaling.
Product image
Safer decision-making checklist before using BPC-157
When someone asks me, “Should I try BPC-157?”, the best answer is a process—not a yes/no. Here’s the checklist I use to reduce avoidable risk and make the decision more informed.
1) Screen for red flags
- Unexplained weight loss, persistent fevers, night sweats
- Unexplained bleeding or new abnormal discharge
- New persistent lumps or progressive pain
2) Review medical history and medications
- Any cancer history or active evaluation for malignancy
- Immunosuppressive therapies or complex autoimmune conditions
- Current meds that affect blood vessels, clotting, or inflammation
3) Use a conservative approach
- Start with minimal exposure and short evaluation windows.
- Track side effects with dates and severity.
- Stop and get clinical input for any concerning or worsening symptoms.
4) Don’t let “angiogenesis” become your only metric
If your goal is tissue repair, also track functional outcomes (pain, range of motion, performance metrics) instead of focusing solely on mechanistic chatter like bpc 157 angiogenesis. Real-world results matter more than the story.
FAQ
Does BPC-157 cause cancer by increasing angiogenesis?
No one can say that confidently from human evidence alone. The concern is theoretical because angiogenesis can support tumor growth, and BPC-157 has been discussed in relation to healing pathways that may intersect with angiogenesis signaling. The responsible stance is to avoid absolutist claims and be especially cautious if you have cancer history or unexplained symptoms.
What BPC-157 side effects should make me stop and seek medical care?
Stop and seek medical attention for serious or persistent symptoms such as unexplained weight loss, ongoing unexplained bleeding, rapidly worsening pain, new persistent lumps, fevers/night sweats, or any significant deterioration in overall condition.
Is bpc 157 angiogenesis relevant for people using it only for recovery or gut issues?
Mechanistically, it can be relevant in the sense that the same signaling networks involved in healing can overlap with angiogenesis. Practically, the real question is whether the human exposure and duration meaningfully change risk—data is limited. That’s why baseline screening and conservative use matter.
Conclusion
BPC-157 discussions often spotlight recovery, but the most important safety upgrade is to face the cancer-related “angiogenesis” question with realism: there’s no clear human proof of causation, yet the theoretical risk conversation isn’t meaningless either. If bpc 157 angiogenesis is part of your reasoning, pair that mechanistic interest with real-world precautions—baseline screening, conservative exposure, symptom tracking, and clinical input when risk factors exist.
Next step: Write down your current health context (diagnoses, red flags, medications, and your main goal), then run a conservative trial plan with clear stop conditions and symptom logs—before you commit to longer use.
Discussion