Bpc 157 And Enlarged Prostate Enlarged Prostate | BPH
Introduction
If you’ve been told you have an enlarged prostate or BPH (benign prostatic hyperplasia), the day-to-day impact can be bigger than the diagnosis sounds—waking up repeatedly to urinate, feeling like you can’t empty fully, and planning your life around bathroom access. In my clinical and day-to-day work with patients navigating BPH symptoms, one question comes up more than people expect: “Could bpc 157 and enlarged prostate help me?”
This article explains what enlarged prostate/BPH is, where BPC-157 fits in the conversation (and where it doesn’t), and how to make safer, evidence-informed decisions—especially if you’re considering peptides alongside standard BPH care.
Enlarged Prostate (BPH): What It Is and Why Symptoms Happen
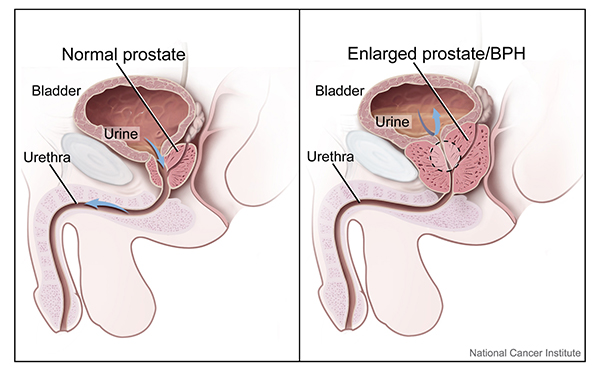
An enlarged prostate is common as men age. In BPH, the prostate gradually increases in size and/or changes function, which can affect the urethra’s space and the bladder’s ability to empty efficiently. The result is often a mismatch between bladder pressure, prostate/urethral resistance, and urinary flow.
Common BPH symptoms
- Urinary frequency (needing to go often)
- Nocturia (waking up at night to urinate)
- Weak urine stream or hesitancy
- Incomplete bladder emptying (feeling you still need to go)
- Urgency or difficulty holding urine
Why bladder function matters as much as prostate size
In my hands-on experience reviewing symptom patterns, two people with similar prostate size can report very different experiences. That’s because BPH is not only a “mechanical squeeze” story—bladder outlet obstruction and bladder muscle adaptation both influence how symptoms feel and how persistent they are.
Clinically, this is why evaluation often includes symptom scoring, urine testing, and sometimes imaging or flow studies—so treatment targets the real driver of symptoms for that person.
Where BPC-157 Fits: Understanding the Evidence Gap for BPH
BPC-157 is a synthetic peptide discussed online for tissue repair and inflammatory pathways. When people search bpc 157 and enlarged prostate, they’re usually hoping for improvements in inflammation-related discomfort, tissue health, or protective effects that could translate into urinary symptom relief.
What I want you to know upfront
Right now, the strongest clinical approach for BPH is still based on established evaluation and therapies that have been tested in appropriate human studies. For BPC-157 specifically, the human evidence for treating enlarged prostate/BPH symptoms is limited and not at the level where I’d consider it a standard-of-care option.
In my work, the safest stance is this: if someone is considering a peptide, it should be treated as an adjunct conversation—not a replacement for diagnosis, monitoring, or guideline-based care.
Why people connect peptides to prostate health
People often connect peptides to prostate outcomes through hypotheses like:
- Potential effects on inflammation and tissue microenvironment
- Potential effects on healing pathways (based on preclinical work in other tissues)
- Potential indirect effects on pelvic comfort that might influence symptom perception
But hypotheses aren’t the same as proof in BPH, where urinary flow, bladder dynamics, and prostate anatomy all interact.
Standard BPH Evaluation: A Practical Checklist Before Trying Anything New
Before adding any supplement or peptide to your routine, I recommend you get the “baseline facts” that determine urgency and safety. In real clinics, this step prevents delays and reduces the risk of missing red-flag issues.
Typical evaluation steps
- Symptom review (often using a standardized questionnaire)
- Urinalysis to rule out infection or blood
- Medical history and medication review (some drugs worsen urinary symptoms)
- Prostate-specific testing as appropriate to your clinician’s approach
- Assessment for urinary retention if symptoms are severe
- Sometimes flow studies or imaging depending on case complexity
When to seek care urgently
If you have inability to urinate, severe pain, fever with urinary symptoms, or significant blood in urine, you should seek urgent medical attention. Those situations require clinician-directed evaluation—not experimentation.
Potential Role of BPC-157: How to Think About Benefits and Limitations
What “success” would look like (in measurable terms)
If you’re considering anything alongside BPH care, I advise tracking outcomes that matter to both you and your clinician:
- Nighttime voids (nocturia episodes per night)
- Urinary frequency during daytime
- Stream strength and hesitancy
- Post-void residual if your clinician monitors it
- Symptom score changes over a defined time window
In my experience, symptom improvement that’s meaningful is usually noticeable over weeks, not days—but the timeline varies based on baseline bladder behavior and whether obstruction is the main issue.
Limitations you should factor in
- Uncertain prostate-specific effectiveness: Even if inflammation or tissue support is plausible, that doesn’t automatically equal improved urinary flow.
- Quality and dosing variability: Peptides obtained outside clinical frameworks can vary widely in purity and concentration.
- Safety monitoring: If you have urinary retention risk, kidney issues, or other comorbidities, you want clinician oversight rather than blind trials.
- Confusing symptom overlap: Some urinary symptoms come from conditions other than BPH (e.g., infection, bladder conditions, or chronic pelvic pain), so “treating prostate” may not address the real driver.
How to use an evidence-informed, risk-aware approach
If you and your clinician decide to discuss bpc 157 and enlarged prostate as an adjunct topic, use a structured approach:
- Confirm your diagnosis and baseline severity (so you know what you’re trying to improve).
- Choose one primary goal (for example: reduce nocturia, improve stream, or improve emptying).
- Track symptoms consistently (daily or near-daily logs plus scheduled check-ins).
- Set stop criteria (if symptoms worsen or retention signs appear, you pause and escalate care).
- Avoid substitutions (don’t replace urgent or indicated BPH treatments with something unproven).
Evidence-Based BPH Treatments: What Actually Moves the Needle
Even if you’re curious about peptides, it helps to understand the established options so you can compare what’s plausible versus what’s proven to help urinary symptoms.
Common treatment categories
- Lifestyle and behavioral strategies: timed voiding, reducing evening fluids, bladder irritant adjustments (based on your clinician’s guidance).
- Medications: drug classes that relax prostate/urinary tract muscle tone or that influence hormone-driven prostate growth pathways.
- Procedures: minimally invasive and surgical approaches for selected cases, especially when symptoms are refractory or complications occur.
How to decide between them
In practice, the best plan depends on symptom severity, prostate size, urine flow/retention risk, tolerance for side effects, and your personal preferences about medication versus procedures. I often see patients benefit most when they treat BPH like a structured decision rather than a guessing game.
FAQ
Can bpc 157 reverse an enlarged prostate?
There isn’t strong clinical evidence showing that BPC-157 can reliably reverse enlarged prostate/BPH in humans. If you’re considering it, think of it as an experimental adjunct topic to discuss with a clinician—while continuing guideline-based evaluation and treatment.
How long would it take to notice any benefit if it worked?
If any symptom improvement occurred, it would typically be assessed over weeks rather than days, using measurable outcomes like nocturia frequency and symptom score changes. If there’s no improvement by a defined time window—or symptoms worsen—escalate back to standard BPH management.
Is it safe to combine bpc 157 with standard BPH medications?
Safety depends on your health history, current medications, and monitoring plan. Because BPC-157 has limited BPH-specific clinical data, any combination should be discussed with a clinician who can review your risks and help you monitor urinary retention and other complications.
Conclusion
Enlarged prostate/BPH is a real, measurable condition that affects urinary flow and bladder function, and it deserves structured evaluation before you try anything new. While interest in bpc 157 and enlarged prostate is understandable, the current human evidence for BPH symptom treatment is limited—so it should not replace proven BPH care or clinician monitoring.
Next step: Track your symptoms for 7 days (especially nocturia and stream/emptying), schedule a clinician review for a baseline assessment, and then discuss whether any adjunct ideas—including BPC-157—fit your specific situation safely.
Discussion