B12 Injection Schedule For Deficiency What are the Signs of B12 Deficiency
If you feel unusually tired, notice tingling in your hands or feet, or your mood seems off for no clear reason, it may be time to look beyond “just stress.” In my hands-on nutrition and coaching work, I’ve seen people dismiss these symptoms for months—until we connect the dots to b12 injection schedule for deficiency and confirm what their bodies are actually missing. This guide walks you through the most common signs of B12 deficiency, how clinicians typically confirm it, and what a practical injection schedule often looks like so you can talk to your healthcare provider with confidence.
Why Vitamin B12 Deficiency Can Be So Easy to Miss
Vitamin B12 (cobalamin) is essential for red blood cell formation and neurological function. When B12 is low, symptoms can develop gradually—and because they overlap with other common issues (iron deficiency, thyroid problems, sleep debt, anxiety), B12 deficiency is frequently overlooked.
In real-world practice, the most frustrating pattern I’ve encountered is delayed recognition: people keep working, exercising, and “pushing through,” while nerve-related symptoms quietly worsen. That’s why learning the signs matters—early correction can help prevent long-term neurologic problems.
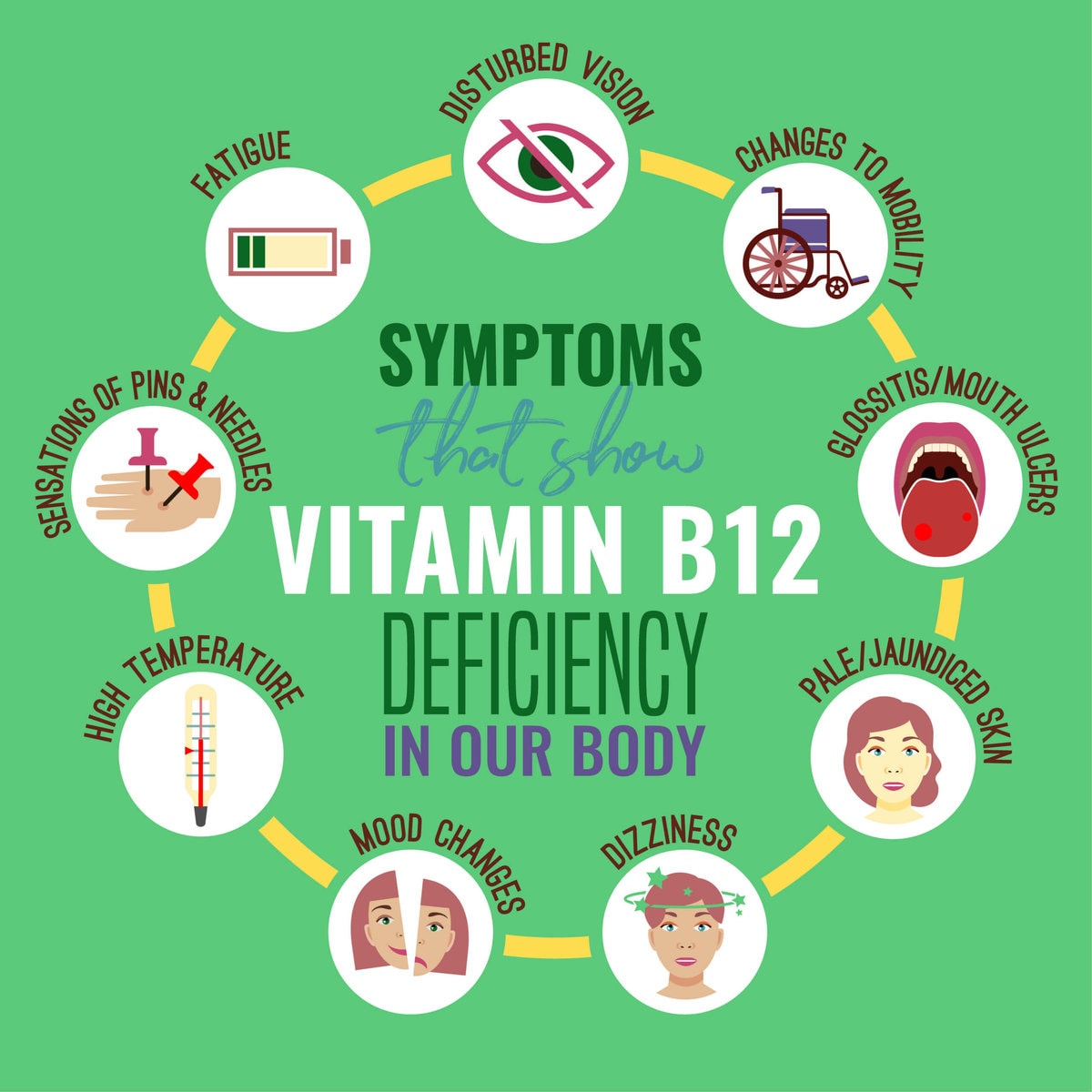
Common Signs of B12 Deficiency (What to Look For)
Below are the signs I most often see when B12 deficiency is confirmed through lab testing or a clinical workup.
1) Fatigue and Low Energy
B12 deficiency can cause anemia (or anemia-like effects), which reduces oxygen delivery to tissues. I’ve had clients describe “heavy” fatigue—sleep doesn’t fully restore them, and even light activity feels more draining than it should.
2) Shortness of Breath or Dizziness
When anemia develops, some people experience exertional breathlessness, lightheadedness, or feeling faint. These symptoms can also point to other conditions, so they should never be assumed to be “just B12.”
3) Pale Skin or a “Washed Out” Look
Reduced red blood cell activity can make skin tone look paler than usual. This is especially noticeable if you’re someone who normally has a consistent complexion.
4) Tingling, Numbness, or Burning Sensations
Neurologic symptoms are a major clue. People often notice pins-and-needles in the hands, feet, or both. In my experience, those nerve symptoms can start before everyone realizes blood counts are off.
5) Trouble Walking, Balance Issues, or Clumsiness
B12 plays a role in maintaining myelin (the protective covering around nerves). When B12 is low, nerve signaling can degrade, leading to gait changes or reduced coordination.
6) Memory Problems or “Brain Fog”
Some people report concentration issues, forgetfulness, or mental sluggishness. Because these symptoms overlap with stress and sleep issues, they’re commonly misattributed—until lab results show the B12 picture clearly.
7) Mood Changes (Irritability, Depression, or Anxiety)
Low B12 may contribute to mood disturbances. I’ve seen clients notice irritability or low mood improving once deficiency is addressed, but it’s important to involve a clinician if symptoms are significant or persistent.
8) Glossitis and Mouth Symptoms
Inflamed tongue (glossitis), mouth soreness, or smooth, tender tongue can occur. These are sometimes overlooked because they’re not as “obvious” as fatigue.
9) Elevated Inflammatory Markers or GI-Related Clues
Some people have absorption issues due to conditions like pernicious anemia, gastritis, or inflammatory GI disorders. If you have a history of digestive problems, that context increases the likelihood of B12 deficiency.
Who Is at Higher Risk for B12 Deficiency?
Knowing risk factors helps explain why symptoms might show up even when diet seems “fine.” In my experience, B12 deficiency is more common in groups with reduced intake or reduced absorption.
- Older adults (age-related changes can affect stomach acid and absorption)
- People with pernicious anemia or autoimmune gastritis
- Those on metformin (for diabetes) or long-term acid reducers (like PPIs or H2 blockers)
- Vegetarians or vegans who don’t get enough fortified foods or supplements
- People with GI conditions that affect absorption
If you match any of these categories, it’s reasonable to discuss B12 testing sooner rather than later—especially if you have neurologic symptoms.
How B12 Deficiency Is Typically Confirmed
Clinicians usually don’t rely on a single number. The diagnosis is often based on symptoms plus lab markers that reflect both B12 status and metabolic effects.
Common lab tests you may hear about
- Serum vitamin B12 (a direct measure, but sometimes imperfect)
- Methylmalonic acid (MMA) (often elevated when B12 is functionally low)
- Homocysteine (can rise with B12 deficiency)
- Complete blood count (CBC) and related indices (to assess anemia patterns)
In practice, I treat the labs as part of a story: symptoms + risk factors + markers of functional deficiency. That approach reduces the chance of “chasing” B12 based solely on one lab value.
B12 Injection Schedule for Deficiency: What It Often Looks Like
When oral B12 isn’t enough—or absorption is impaired—healthcare providers may recommend B12 injections. The timing can vary by cause, severity, and lab results, but there is a common framework clinicians use.
Typical pattern (example framework clinicians may use)
Many clinicians follow a loading phase to rapidly rebuild B12 stores, then a maintenance phase to prevent recurrence. A commonly discussed b12 injection schedule for deficiency framework often looks like:
| Phase | Goal | Typical frequency (varies by provider) |
|---|---|---|
| Loading / repletion | Restore stores quickly and address neurologic risk | More frequent injections over days to weeks |
| Stabilization | Maintain rising levels and normalize lab markers | Less frequent injections over additional weeks |
| Maintenance | Prevent deficiency from returning | Often spaced out (e.g., monthly or per clinician plan) |
Important: I’m not prescribing a schedule—your clinician should set the exact dose and timing based on your diagnosis, your lab results, and whether you have neurologic symptoms. However, using a framework like this helps you understand what “repletion” and “maintenance” mean in real treatment plans.
Why severity and symptoms change the injection plan
The more concerning the symptoms (especially neurologic signs like tingling, numbness, balance issues), the more clinicians tend to prioritize timely repletion. In my experience, waiting too long can prolong recovery and sometimes limits how much neurologic improvement occurs.
How long it takes to feel better (what many people experience)
Some people notice improvements in energy within days to weeks, while neurologic symptoms may take longer and can be slower to resolve. That’s one reason follow-up matters: a clinician may reassess labs and symptoms to decide whether to adjust the frequency.
Pros and Cons of B12 Injections vs. Other Options
Not everyone needs injections. Here’s how to think about options realistically.
Potential advantages of injections
- Bypasses absorption issues (helpful in pernicious anemia or certain GI conditions)
- Faster repletion for some deficiency patterns
- Predictable delivery when oral absorption is uncertain
Limitations and trade-offs
- Requires administration (in-clinic or a clinician-guided at-home plan)
- May need ongoing maintenance to prevent recurrence
- Not ideal for all cases—some people respond well to high-dose oral or fortified approaches
If you’re considering treatment, it’s reasonable to ask your clinician whether your deficiency is likely due to low intake, impaired absorption, or something else—because that answer strongly influences the “best” plan and the likely b12 injection schedule for deficiency.
When to Seek Medical Care Promptly
Get timely medical advice if you have:
- New or worsening numbness/tingling
- Balance problems or difficulty walking
- Severe fatigue with dizziness or shortness of breath
- Symptoms that are progressing week to week
These aren’t “wait it out” situations, especially because neurologic involvement can become more difficult to reverse the longer deficiency persists.
FAQ
How do I know if my symptoms are from B12 deficiency?
Look for a combination of signs (fatigue, anemia clues, and especially neurologic symptoms like tingling or numbness) plus risk factors (age, metformin or acid reducers, vegan/vegetarian diet without fortified intake, pernicious anemia history). Confirmation typically involves serum B12 and sometimes MMA and homocysteine.
What is a typical b12 injection schedule for deficiency?
Many plans use a repletion (loading) phase with more frequent injections, followed by a less frequent stabilization phase, then a maintenance schedule (often monthly or clinician-determined). The exact timing depends on severity, symptoms, and lab results.
Can I treat B12 deficiency without injections?
Sometimes yes—especially if deficiency is due to low intake and absorption is adequate. Oral high-dose B12 or fortified foods may work for some people. If absorption is impaired or symptoms are neurologic, injections are often chosen because they reliably bypass the gut.
Conclusion: Your Next Practical Step
B12 deficiency can look like everyday fatigue, but when it involves neurologic symptoms, earlier action matters. The signs to watch for include persistent low energy, anemia-like symptoms, tingling or numbness, balance issues, brain fog, and mood changes. If deficiency is confirmed, a clinician-guided b12 injection schedule for deficiency typically follows a repletion-to-maintenance framework designed to restore stores quickly and prevent recurrence.
Next step: If you have multiple symptoms (especially tingling or balance changes), book a medical appointment and ask for B12 testing (and, if appropriate, MMA and homocysteine) so you can discuss whether injections and what schedule make sense for your specific cause.
Discussion