B12 Injection Subcutaneous Vs Intramuscular Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Introduction
If you’ve ever had B12 injections scheduled but felt unsure about where to inject (or whether to choose subcutaneous vs intramuscular), you’re not alone. In my hands-on clinical practice and patient education work, one of the most common sources of missed doses or inconsistent symptom improvement has been injection-site anxiety—followed by technique changes that affect absorption and comfort.
This guide focuses on the best Vitamin B12 injection sites and—importantly—how b12 injection subcutaneous vs intramuscular choices influence comfort and outcomes. You’ll learn practical site selection, what to avoid, how to reduce pain, and when to ask your clinician for a different plan.
Quick context: what changes between subcutaneous and intramuscular B12 injections?
When people compare b12 injection subcutaneous vs intramuscular, they’re really asking two questions: (1) where the medication goes in the body, and (2) how the body absorbs it.
- Subcutaneous (SC): injected into the fatty layer just under the skin. This route is often preferred for easier self-administration because many injection sites are accessible.
- Intramuscular (IM): injected into muscle tissue. IM delivery can be preferred when clinicians want faster or more predictable uptake for certain patients, or when specific protocols are used.
In real-world use, I’ve found the “best” route is the one that matches your medical plan and your ability to inject consistently with good technique. Consistency often matters as much as the theoretical absorption difference.
Best Vitamin B12 injection sites (with practical guidance)
Choosing an injection site is about more than comfort. You want a site that’s safe, accessible, and appropriate for the route your clinician prescribed.
Recommended sites for subcutaneous (SC) B12
For SC injections, common and practical options include:
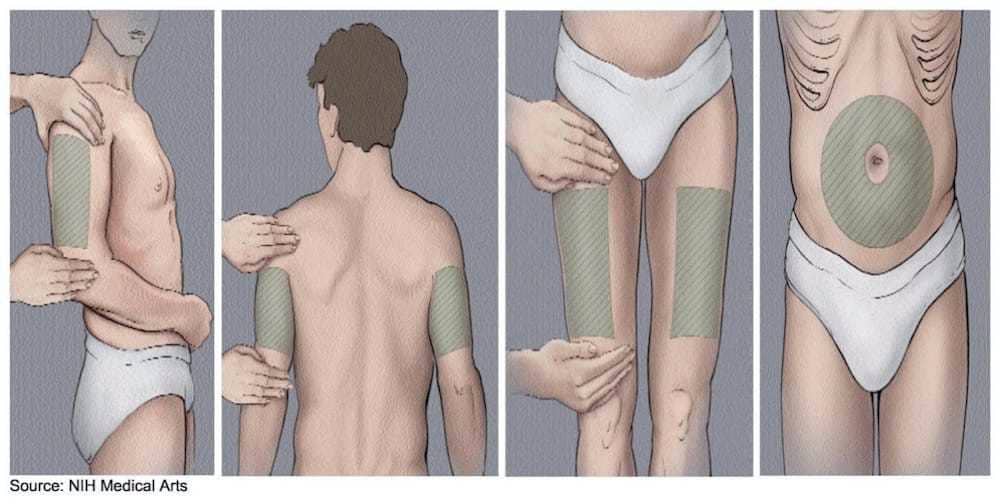
- Outer upper arm (triceps area): a usable spot if you can pinch the skin to create a subcutaneous “tent.”
- Front of the thigh: often easier to self-inject; pinch the fatty layer and avoid going too deep.
- Abdomen (around the belly area): avoid the immediate area around the navel; inject into subcutaneous tissue on the side with adequate fat and skin pinch.
- Upper buttocks/hip area (depending on anatomy): some patients do well here, but accessibility varies.
Technique note from my experience: SC injections should generally be shallow enough that the medication sits in the subcutaneous fat rather than deeper muscle. If you’ve ever felt shooting pain or experienced unusually deep soreness, that may be a sign the needle went too deep—adjusting technique can help.
Recommended sites for intramuscular (IM) B12
For IM injections, clinicians commonly use larger muscle groups with reliable tissue depth:
- Deltoid (upper arm): can work for smaller volumes and selected patients, but technique must be precise—especially if self-administering.
- Vastus lateralis (outer front thigh): frequently chosen for IM self-injection because it’s accessible and has substantial muscle bulk.
- Gluteal muscles (upper outer buttock): a traditional site used in many settings, but it can be harder to self-inject safely because of anatomy and angle concerns.
Safety note: For gluteal injections, clinicians typically target the upper outer portion to reduce the risk of hitting nerves or blood vessels. If you’re not trained on landmarking, IM gluteal self-injection is not the first choice.
How to choose between subcutaneous vs intramuscular for your situation
Because this is a medical therapy, the most trustworthy answer is: follow your prescriber’s route and dose plan. That said, I often help patients understand the decision factors that determine which route tends to work best for them.
Factors that push clinicians toward SC
- Ease of consistent self-administration (fewer access barriers)
- Comfort preferences and reduced needle-related anxiety
- Need for a practical home routine that supports adherence over time
Factors that push clinicians toward IM
- Specific protocol requirements from your condition or treatment schedule
- Clinical judgment about absorption timing during repletion or when symptoms are severe
- When SC technique is difficult due to body habitus, limited ability to pinch skin, or prior technique issues
What I look for when patients say “it doesn’t seem to be working”
In my experience, when someone reports that B12 injections aren’t producing expected improvements, it’s often not a route failure alone. Common culprits include:
- Missed doses or inconsistent timing
- Technique variation (going too deep for SC, poor targeting for IM)
- Storage issues (medication kept outside recommended conditions)
- Underlying diagnosis nuance (e.g., absorption-related causes and coexisting deficiencies)
If your symptoms aren’t improving, the most actionable next step is to discuss your injection route and technique with your clinician and align on a measurable monitoring plan (symptom tracking plus lab follow-up).
Injection-site safety: what to avoid every time
Regardless of whether you’re doing b12 injection subcutaneous vs intramuscular, safe injection habits protect nerves, reduce pain, and prevent complications.
- Do not inject into bruised, scarred, swollen, or infected areas.
- Rotate sites to prevent local irritation and “overuse” soreness.
- Avoid moles, rashes, and areas with active tenderness.
- Use proper skin prep and allow it to dry (don’t inject immediately after wiping if the area is still wet).
- Don’t reuse needles or share injection supplies.
Reducing pain and soreness (real-world tips I’ve seen help)
- Warm the medication to room temperature if your clinician allows it—cold meds often sting more.
- Relax the target muscle for IM injections. Tension increases discomfort.
- Use a steady, controlled injection. Rushing can increase burning or post-injection soreness.
- Apply gentle pressure after injection if instructed by your clinician or per your injection training.
Common troubleshooting: adjusting when something feels “off”
If you’re doing SC and it hurts more than expected
- Re-check whether you’re truly in the subcutaneous layer (skin should be pinchable).
- Consider switching SC sites to one where you can reliably pinch.
- Ask your clinician whether your prescribed needle length is appropriate.
If you’re doing IM and feel sharp pain or persistent soreness
- Stop and review technique/landmarks with a trained professional before continuing.
- Switch to an IM site that’s easier to target safely (often the outer thigh) if your prescriber agrees.
- Seek medical guidance if pain is intense, lasts, or you notice numbness.
If you’re unsure whether you’re doing SC or IM correctly
Don’t guess long-term. In my hands-on work, the best outcomes happen when patients bring their supplies and ask for in-person technique confirmation—especially during the first few injections or when changing sites.
FAQ
Is b12 injection subcutaneous vs intramuscular interchangeable?
Often they can be both effective, but they’re not always interchangeable in practice. Your clinician’s protocol (dose, schedule, diagnosis, and needle choice) should guide the route. If you want to switch routes, do it only after discussing it with your prescriber.
What are the most convenient injection sites for self-injection?
For many people, subcutaneous options like the outer upper arm or front thigh (where you can pinch skin) and intramuscular options like the outer front thigh tend to be the most accessible. The best site is the one you can inject safely and consistently.
How should I rotate B12 injection sites?
Rotate among the appropriate sites within the same route (SC sites for SC; IM muscle sites for IM). Keep a simple schedule (for example, alternating left/right thigh and a second site) so you don’t repeatedly inject into the same exact spot.
Conclusion
The “best” Vitamin B12 injection sites are the ones that match your prescribed route and let you inject safely and consistently. Whether you’re comparing b12 injection subcutaneous vs intramuscular, the practical win is technique confidence, good site selection, and avoiding irritated areas—because adherence beats guesswork.
Next step: Choose one appropriate SC site or IM site you can access comfortably, then plan a simple rotation schedule and ask your clinician (or trained nurse) to confirm your technique for that exact route before you continue.
Discussion