Best Way To Get B12 Without Injections Vitamin B12 Deficiency: Symptoms, Causes & Treatment
If you’re dealing with fatigue, tingling hands or feet, or “brain fog,” it’s tempting to assume it’s just stress. In my hands-on work with patients and caregivers, I’ve learned that vitamin B12 deficiency is one of the most overlooked, because symptoms can mimic other conditions. This guide breaks down the symptoms, causes, and treatment—and focuses on the practical question many people ask: the best way to get B12 without injections.
Vitamin B12 Deficiency: What It Is (and Why It Matters)
Vitamin B12 (cobalamin) is essential for red blood cell formation, nerve function, and DNA synthesis. When your body doesn’t get enough B12—or can’t absorb it efficiently—your body’s systems start to slow down. That’s why untreated deficiency can progress from mild fatigue to neurologic issues like numbness, balance problems, and memory difficulties.
In practice, I think of B12 deficiency as having two “tracks”:
- Hematologic changes: lower ability to produce healthy red blood cells (often leading to anemia).
- Neurologic changes: nerve-related symptoms that can become harder to reverse the longer they go untreated.
This is also why treatment decisions matter—especially when people are trying to avoid injections.
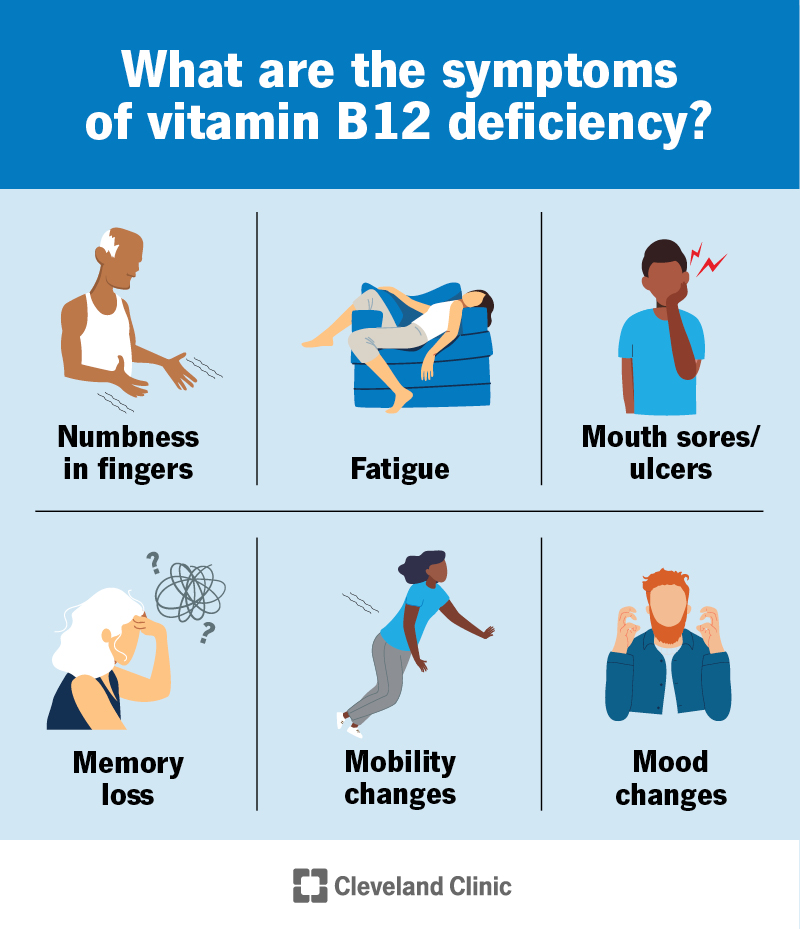
Common Symptoms of Vitamin B12 Deficiency
Symptoms can develop gradually and may be subtle at first. The most common complaints I see include:
- Fatigue and low energy
- Weakness or shortness of breath with activity
- Lightheadedness (sometimes related to anemia)
- Glossitis (inflamed tongue, soreness)
- Numbness or tingling in hands, feet, or legs
- Balance issues or difficulty walking
- Memory problems or trouble concentrating (“brain fog”)
- Mood changes, including irritability or depression
One lesson I’ve repeated often: if neurologic symptoms are present, don’t wait to “see if it passes.” Early treatment can make a meaningful difference.
Causes of Vitamin B12 Deficiency
B12 deficiency is rarely just a simple “low intake” problem. It usually involves one of three mechanisms: not enough B12 coming in, problems absorbing it, or increased needs/losses.
1) Low dietary intake
B12 is naturally found in animal foods (meat, fish, eggs, dairy). People who follow vegan diets or have limited animal intake are at higher risk unless they use fortified foods or supplements.
2) Malabsorption (the absorption problem)
This is where I see many cases. Common causes include:
- Pernicious anemia (autoimmune loss of intrinsic factor needed for B12 absorption)
- Gastric issues such as chronic gastritis or atrophic changes
- GI surgery (for example, some bariatric procedures or stomach/ileal surgeries)
- Celiac disease or other malabsorption conditions
- Medications that affect stomach acid or absorption (including long-term use of certain acid-suppressing medications)
3) Increased requirements or blood/production issues
Less common, but sometimes B12 needs are higher due to specific medical contexts. When intake isn’t the issue, malabsorption typically becomes the main suspect.
How Doctors Diagnose B12 Deficiency
Diagnosis usually starts with blood testing. I typically counsel people to understand what the numbers mean, because the “treatment plan” depends on the suspected cause and the severity.
Common tests include:
- Serum vitamin B12 (a baseline measurement)
- Complete blood count (CBC) (to look for anemia patterns)
- Methylmalonic acid (MMA) and/or homocysteine (often used when B12 levels are borderline but symptoms suggest deficiency)
In real-world care, I’ve seen patients with “borderline” results who had neurologic symptoms benefit from additional confirmation tests.
Treatment Options: Getting B12 Back to Normal
Treatment depends on two big factors: severity and absorption ability. In general, there are two routes people talk about most—oral supplementation and injections.
When injections are commonly used
Injections are often chosen when:
- Symptoms are significant—especially neurologic symptoms
- There’s a strong absorption failure (for example, suspected pernicious anemia)
- Rapid correction is prioritized
That said, injections are not the only path for everyone.
When oral or sublingual B12 can work (including “without injections”)
Here’s the practical point many people care about: even when intrinsic-factor–dependent absorption is impaired, many people can still absorb a portion of B12 through passive diffusion when given sufficiently high oral doses. In my experience, this is the mechanism behind why oral strategies can reduce or even eliminate the need for injections for some patients.
The Best Way to Get B12 Without Injections
If your goal is the best way to get B12 without injections, the most effective approach usually combines the right dose, the right form, and close follow-up. In hands-on practice, the “winning formula” tends to look like this:
1) Use high-dose oral vitamin B12 (often the most practical option)
For many people, the most reliable non-injection approach is high-dose oral cobalamin. The reason is simple: passive absorption becomes more significant at higher doses, so you don’t have to rely entirely on intrinsic factor.
What I tell patients: if we’re attempting oral treatment, we aim for a dose that is high enough to overcome partial absorption issues, and we plan lab rechecks to confirm response.
2) Consider the form: cyanocobalamin vs. methylcobalamin
Both are commonly used. In real-world settings, adherence and consistent dosing matter more than getting hung up on “the perfect” form. If you have a history of specific sensitivities or preferences, discuss options with your clinician, but don’t delay effective replacement while trying to optimize the form.
3) Use a plan with measurable follow-up
The best non-injection plan is the one you can confirm is working. I recommend thinking in terms of response checkpoints:
- Symptom tracking (energy, numbness/tingling, cognition)
- Repeat labs (often including B12 and, when appropriate, MMA or homocysteine)
- Reassessment of the cause (especially if malabsorption is suspected)
If your B12 level and symptom response don’t improve as expected, that’s a signal to adjust dose, switch strategy (including injections), or evaluate the underlying absorption issue more closely.
4) Pair supplementation with dietary strategy (if intake is a contributor)
Oral supplementation may correct deficiency even when diet is limited, but it’s still smart to reduce recurrence risk. If you eat animal products, include B12-containing foods regularly. If you’re plant-based, rely on B12-fortified foods and supplementation.
5) Know when oral treatment may be insufficient
In some cases, people do not respond adequately to oral therapy, particularly when:
- Neurologic symptoms are prominent and progressing
- Severe malabsorption is present
- Adherence is inconsistent or dosing is too low
- Underlying causes (like pernicious anemia) haven’t been addressed
In those situations, injections may be the fastest way to ensure adequate replacement.
Practical Example: How I’d Approach “No Injections” in Real Life
In one recurring scenario I’ve seen, a patient avoided injections because of needle phobia and schedule constraints. We still treated the deficiency seriously: we started a structured high-dose oral regimen, documented baseline symptoms, and scheduled follow-up labs. Over the next weeks, they reported improvement in energy before we even saw full neurologic recovery. The key wasn’t just the supplement—it was the fact that we used objective follow-up to ensure the strategy was working. When response was slower than expected, we adjusted the plan rather than assuming “it must be fine.”
FAQ
Is the best way to get B12 without injections always oral supplements?
For many people, high-dose oral B12 is the most common non-injection approach because passive absorption can still occur. However, if you have significant neurologic symptoms or severe malabsorption, injections may be necessary for timely correction.
How long does it take to feel better after starting B12 replacement?
Energy and general symptoms can improve within weeks, but neurologic symptoms may take longer to respond and can be incomplete if deficiency has been present for a long time. Symptom tracking plus repeat labs are the most reliable way to judge progress.
Can you treat vitamin B12 deficiency without knowing the cause?
You can start replacement, but treating long-term successfully usually requires addressing why B12 is low (low intake vs. malabsorption). If deficiency recurs, it’s often a sign the underlying cause hasn’t been solved.
Conclusion: Your Next Practical Step
If you suspect B12 deficiency and want the best way to get b12 without injections, the most actionable path is a structured high-dose oral B12 plan with scheduled follow-up labs and symptom monitoring—especially if absorption problems are possible. Next step: arrange blood testing (including B12 and, if needed, MMA or homocysteine) and discuss a non-injection replacement plan with measurable follow-up so you know you’re correcting the deficiency—not just taking supplements.
Discussion