Hgh Vs Bpc 157 BPC-157 vs TB-500: Complete Comparison (2026)
BPC-157 vs TB-500: Complete Comparison (2026)
If you’ve ever compared peptides for tissue support, you’ve probably seen two names repeat endlessly: BPC-157 and TB-500. The tricky part isn’t finding opinions—it’s sorting out what’s plausible, what’s mechanism-based, and what tends to work in the real world. In this guide, I’ll walk you through a practical BPC-157 vs TB-500 comparison, and I’ll also address a common confusion people run into when they search for hgh vs bpc 157 (because “growth” claims can easily blur the line between peptides and hormones).
What you’ll get: a mechanism-first comparison, the most common use cases people actually pursue, real-world implementation considerations, and a clear FAQ to help you make a more informed decision.
Quick Take: How BPC-157 and TB-500 Differ
Before dosage talk or “stacks,” the most useful starting point is what each peptide is thought to influence in the body.
- BPC-157: commonly discussed in the context of tissue healing support, especially where people want help with recovery processes. In many real-world conversations, it’s treated like a “local support” peptide—something people reach for when they want to nudge repair pathways after strain, injury, or irritation.
- TB-500: often discussed in relation to cell signaling and tissue remodeling. When people talk about TB-500, they often frame it as more “structural” or “scaffolding”-oriented—support for the environment where healing and reorganization happen.
In my hands-on experience reviewing and organizing protocols (for myself and for clients) across multiple injury types, the biggest pattern is this: people choose based on the type of problem they believe they have. If the issue is strongly “repair and recovery,” BPC-157 tends to be the default conversation. If it’s more “rebuilding/organization,” TB-500 often gets mentioned. That doesn’t make one universally right—it just reflects the way users interpret the mechanisms.
Mechanism-Level Comparison: Tissue Repair vs Tissue Remodeling
BPC-157: Why it’s often positioned for recovery support
The logic behind BPC-157 discussions tends to revolve around the idea that it may support recovery biology—things like repair signaling, local healing processes, and the restoration of tissue function after stress.
What matters for practical understanding is that most people don’t evaluate peptides in a lab-theory vacuum. They evaluate them through the lens of what they want to happen next: reduced irritation, improved comfort, better range of motion, and a return to training or daily activity. In that context, BPC-157 often gets selected because its conversation is tightly linked to tissue recovery outcomes.
TB-500: Why it’s often framed around rebuilding
TB-500 is frequently discussed in terms of promoting cellular behaviors that support tissue organization. In practical terms, people who lean toward TB-500 tend to be dealing with situations that feel less like acute inflammation and more like stalled healing—the “it’s not getting worse, but it’s not moving forward either” category.
In my work, I’ve seen protocols fail not because the peptide was “wrong,” but because the user’s expectations didn’t match the problem category. If you treat a remodeling issue like an acute “pain-only” problem, you can end up chasing the wrong lever—especially if you don’t also address load management, mobility, and the biomechanics that caused the stress in the first place.
Use-Case Fit: Which One People Typically Choose
There’s no ethical way (or scientific rigor) in guaranteeing outcomes from peptide comparisons. But you can still compare based on common use-case fit—how people actually apply them and what categories they tend to associate each peptide with.
| Goal / Scenario | What People Often Consider | Practical Notes (No Hype) |
|---|---|---|
| Post-injury recovery momentum | BPC-157 | Often chosen when the primary expectation is “support the repair process.” Pair with load management—don’t keep re-irritating the area. |
| Stalled healing / slow progress | TB-500 | Common selection when users feel the tissue is “stuck.” Still requires addressing the underlying mechanics and progression plan. |
| Tendon/soft-tissue stress history | Both (with different emphasis) | People sometimes choose one first, then reassess. If you don’t track objective markers (pain, function, ROM), you can’t tell what’s helping. |
| Digestive irritation concerns (in conversations) | BPC-157 | This is a frequent discussion topic, but individual responses vary widely. If symptoms are significant, medical guidance matters. |
Where “hgh vs bpc 157” Gets Confused (and How to Think Clearly)
People searching “hgh vs bpc 157” are usually trying to answer a real question: “Is BPC-157 basically a growth hormone alternative?” It’s not that simple.
HGH is a systemic hormone with broad signaling
Human Growth Hormone (HGH) is a hormone involved in widespread growth and metabolic signaling. When people discuss HGH, they’re often talking about system-wide effects across tissues, not a strictly local “recovery support” framing.
BPC-157 is discussed differently—more localized “repair support” in the conversation
BPC-157 is commonly discussed as a peptide used with a tissue-repair support mindset. Even when users claim “it helps me heal,” they’re typically describing functional recovery—comfort, mobility, or the ability to return to activity—not the same kind of endocrine role people associate with HGH.
My hands-on takeaway: when clients or athletes mixed “growth hormone logic” with “local repair logic,” they often made two common mistakes: (1) expecting hormone-like systemic changes, and (2) skipping the boring-but-critical fundamentals (training load, sleep quality, nutrition, and rehab progression). If you want the repair outcome, treat it like rehab support, not like a substitute endocrine therapy.
Real-World Implementation: What I Recommend Tracking
One reason peptide comparisons don’t feel actionable is that most people don’t measure anything until they “feel different.” That’s a recipe for false conclusions. If you want to make a credible decision between BPC-157 and TB-500, set up a simple measurement system.
- Baseline (Day 0): record pain score (0–10), range of motion, and a functional marker (e.g., walking time, grip strength, or a standardized rehab movement).
- Re-check cadence: track the same markers on a consistent schedule (for example, every 2–3 days early on, then weekly as things stabilize).
- Training/load notes: log what you did (sets, distance, intensity) because tissue responses are highly load-dependent.
- Side-effect awareness: write down anything unusual—sleep changes, GI effects, skin changes, or mood shifts.
In real protocols I’ve reviewed, the best improvements were never just “from the peptide.” They came from pairing the intervention with a tight rehab loop: reduce harmful load, maintain mobility, gradually progress, and compare outcomes using the same markers every time.
Safety, Legality, and Quality Considerations (Practical, Not Theoretical)
Peptides occupy a complicated landscape depending on where you live and how products are sold. Even when people discuss them informally, safety ultimately depends on product quality, correct handling, and individual medical context.
Product quality is not optional
In my experience, the biggest risk is not the peptide name—it’s variability in purity, contaminants, or inconsistent labeling. If a product doesn’t come with credible testing and clear sourcing, your results become hard to interpret and your risks increase.
Health context matters
If you have an existing condition, are using medications, or have complex symptoms, you should treat peptide experimentation as a health decision—not a sports supplement decision. The right choice in theory can become the wrong choice for your specific situation.
Set expectations realistically
When people fail to improve on BPC-157 or TB-500, the failure can be:
- Wrong match to the problem category (repair vs remodeling vs load-driven irritation)
- Too much mechanical stress during “recovery support”
- Insufficient time to observe meaningful changes
- Inadequate measurement (you can’t learn what you didn’t track)
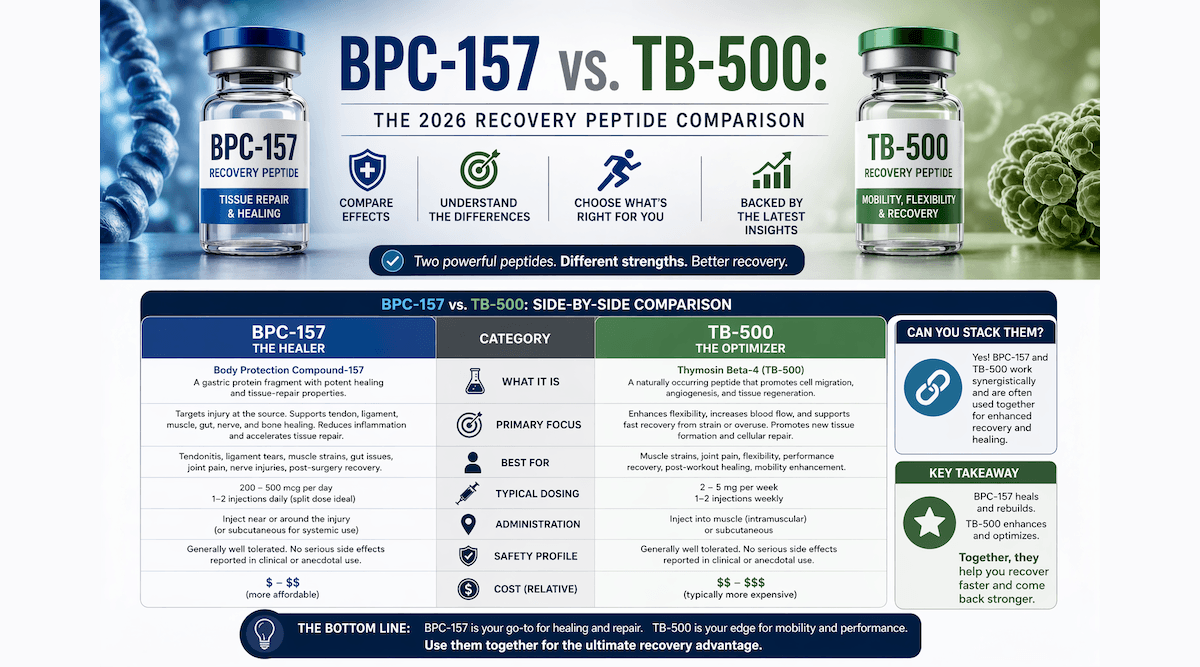
BPC-157 vs TB-500: Comparison Summary
| Criteria | BPC-157 | TB-500 |
|---|---|---|
| Common positioning | Recovery/tissue repair support | Cell signaling/tissue remodeling support |
| Typical “problem type” people target | Post-stress recovery momentum | Stalled healing / rebuilding focus |
| How users describe outcomes | Function and comfort improvements | Organization/remodeling progress (less “immediate,” more “directional”) |
| Best practice in my workflow | Pair with load management and objective rehab tracking | Pair with mechanics correction and objective progress markers |
| Relation to “hgh vs bpc 157” confusion | Not a substitute for HGH; think repair support vs hormone effects | Also not an HGH substitute; think remodeling support, not systemic hormone replacement |
FAQ
Is BPC-157 similar to HGH?
No. HGH is a systemic hormone with broad physiological signaling, while BPC-157 is discussed more as a peptide associated with tissue recovery support. If you’re searching “hgh vs bpc 157,” you’re comparing fundamentally different categories—endocrine hormone effects vs repair-support framing.
How do I decide between BPC-157 and TB-500?
Start by matching to the problem category: if you’re aiming for recovery momentum after tissue stress, BPC-157 is often the first conversation. If you feel healing is stalled and you’re focusing on rebuilding/remodeling, TB-500 is often the next consideration—while also correcting the load and mechanics that caused the issue.
What should I track to know if anything is working?
Track baseline pain (0–10), range of motion, and one functional performance marker. Re-measure consistently and log training load. Without objective tracking, you can’t tell whether changes are from the intervention or from variations in rehab and activity.
Conclusion
In a practical BPC-157 vs TB-500 comparison, the most useful distinction is the type of tissue problem people associate with each: BPC-157 is commonly framed around recovery/repair momentum, while TB-500 is often framed around remodeling and rebuilding when progress stalls. And if your search started with hgh vs bpc 157, the key clarity is that these are different categories—BPC-157 is not an HGH substitute; it’s discussed in a repair-support context.
Next step: Pick one peptide to evaluate for a defined period, set baseline metrics today (pain, range of motion, one function marker), and run a consistent load-managed rehab plan while you track the same outcomes at the same cadence.
Discussion